

Endoscopic endonasal approach for suprasellar meningiomas: introduction of a new scoring system to predict extent of resection and assist in case selection with long-term outcome data
- PMID: 32707549
- PMCID: PMC8111689
- DOI: 10.3171/2020.4.JNS20475
Endoscopic endonasal approach for suprasellar meningiomas: introduction of a new scoring system to predict extent of resection and assist in case selection with long-term outcome data
Abstract
Objective: The endoscopic endonasal approach (EEA) has gained increasing popularity for the resection of suprasellar meningiomas (SSMs). Appropriate case selection is critical in optimizing patient outcome. Long-term outcome data are lacking. The authors systematically identified preoperative factors associated with extent of resection (EOR) and determined the relationship between EOR and long-term recurrence after EEA for SSMs.
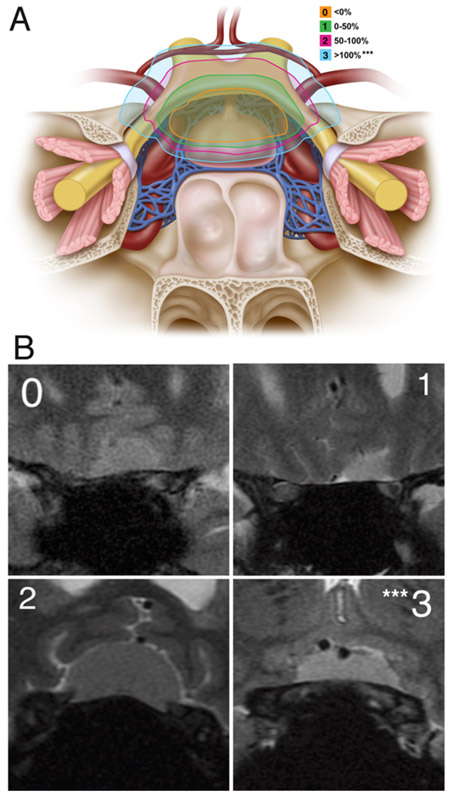
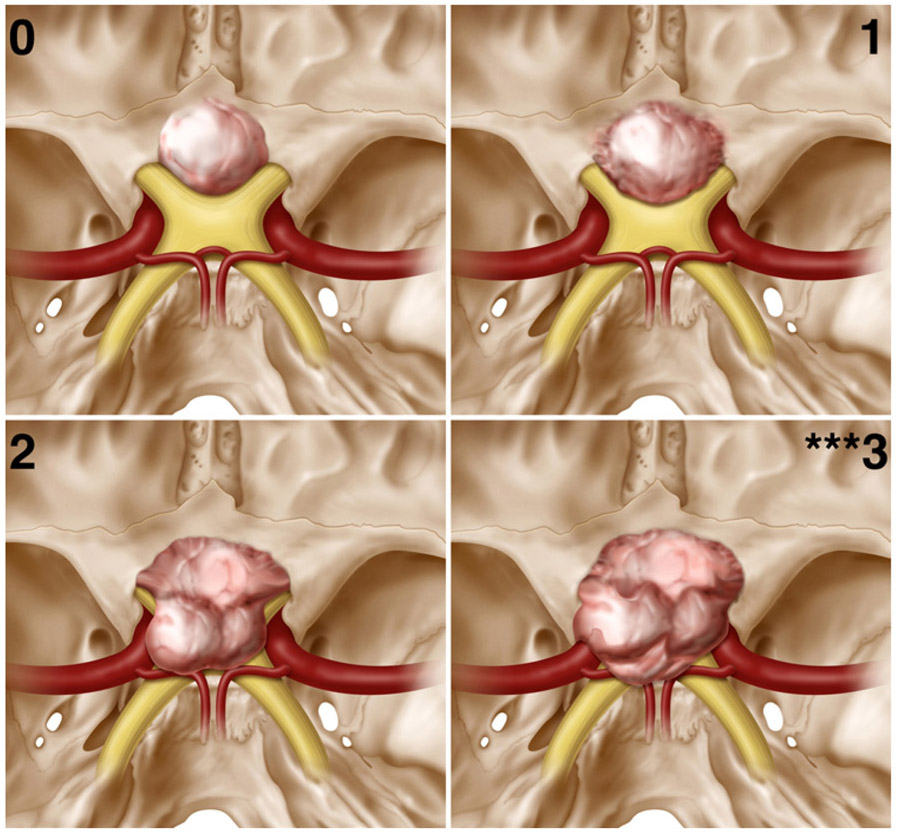
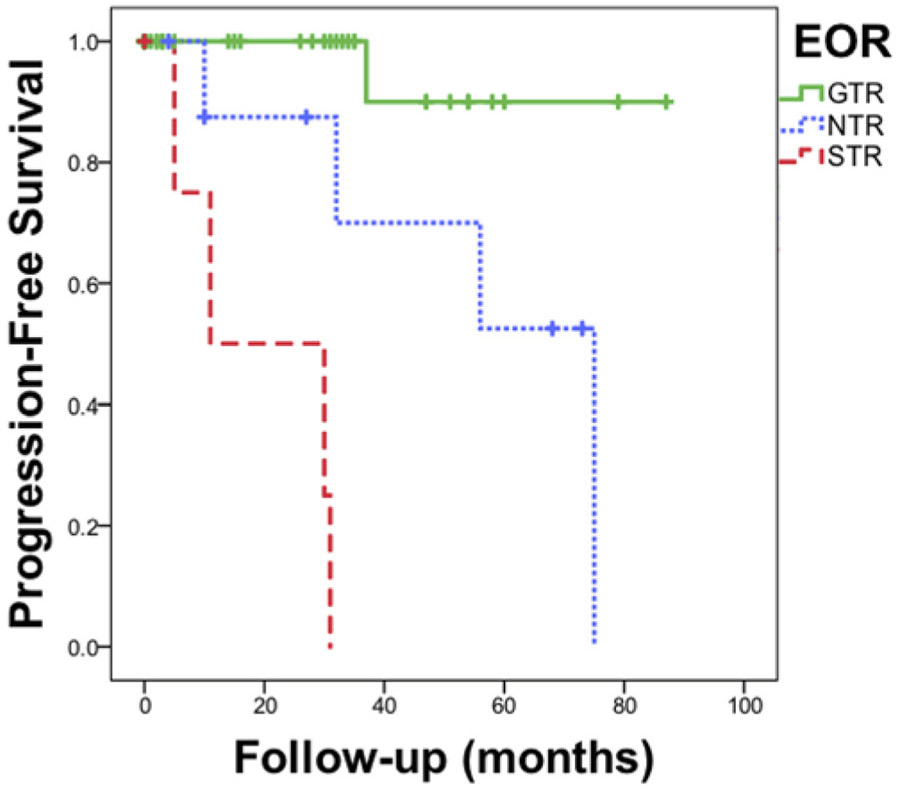
Methods: In this retrospective cohort study, the authors identified preoperative clinical and imaging characteristics associated with EOR and built on the recently published University of California, San Francisco resectability score to propose a score more specific to the EEA. They then examined the relationship between gross-total resection (GTR; 100%), near-total resection (NTR; 95%-99%), and subtotal resection (STR; < 95%) and recurrence or progression with Kaplan-Meier survival analysis.
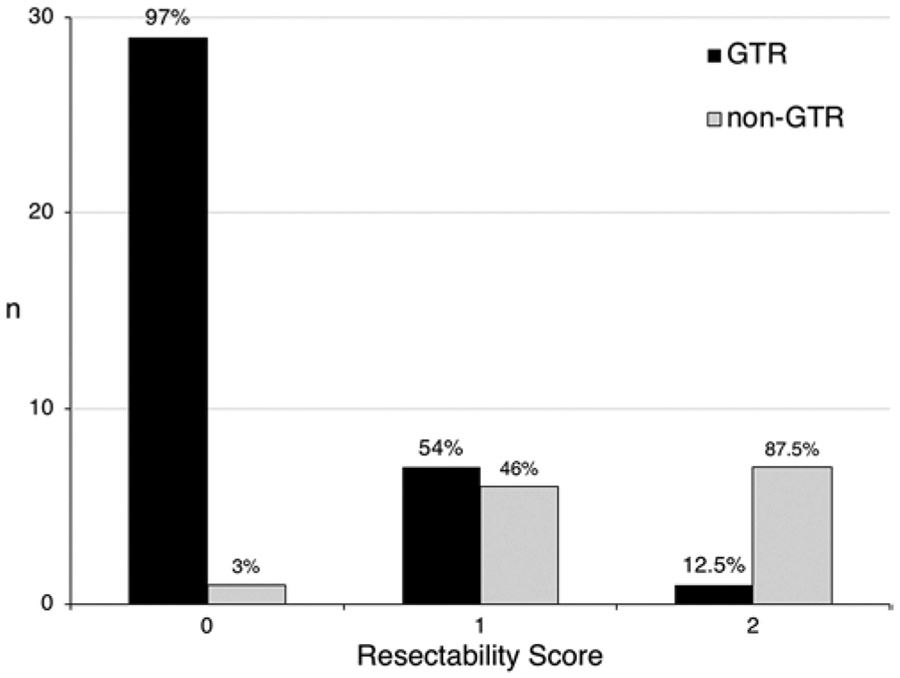
Results: A total of 51 patients were identified. Radiographic GTR was achieved in 40 of 47 (85%) patients in whom it was the surgical goal. Significant independent risk factors for incomplete resection were prior surgery (OR 25.94, 95% CI < 2.00 to 336.49, p = 0.013); tumor lateral to the optic nerve (OR 13.41, 95% CI 1.82-98.99, p = 0.011); and complete internal carotid artery (ICA) encasement (OR 15.12, 95% CI 1.17-194.08, p = 0.037). Tumor size and optic canal invasion were not significant risk factors after adjustment for other variables. A resectability score based on the multivariable model successfully predicted the likelihood of GTR; a score of 0 had a positive predictive value of 97% for GTR, whereas a score of 2 had a negative predictive value of 87.5% for incomplete resection. After a mean follow-up of 40.6 ± 32.4 months (mean ± SD), recurrence was 2.7% after GTR (1 patient with atypical histology), 44.4% after NTR, and 80% after STR (p < 0.0001). Vision was stable or improved in 93.5% and improved in 67.4% of patients with a preoperative deficit. There were 5 (9.8%) postoperative CSF leaks, of which 4 were managed with lumbar drains and 1 required a reoperation.
Conclusions: The EEA is a safe and effective approach to SSMs, with favorable visual outcomes in well-selected cases. The combination of postoperative MRI-based EOR with direct endoscopic inspection can be used in lieu of Simpson grade to predict recurrence. GTR dramatically reduces recurrence and can be achieved regardless of tumor size, proximity or encasement of the anterior cerebral artery, or medial optic canal invasion. Risk factors for incomplete resection include prior surgery, tumor lateral to the optic nerve, and complete ICA encasement.
Keywords: endoscopic endonasal approach; meningioma; planum sphenoidale; skull base; suprasellar; transsphenoidal; tuberculum.
Conflict of interest statement
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
References
-
- Mathiesen T, Kihlström L. Visual outcome of tuberculum sellae meningiomas after extradural optic nerve decompression. Neurosurgery. 2006;59(3):570–576. - PubMed
-
- Ganna A, Dehdashti AR, Karabatsou K, Gentili F. Frontobasal interhemispheric approach for tuberculum sellae meningiomas; long-term visual outcome. Br J Neurosurg. 2009;23(4):422–430. - PubMed
-
- Mahmoud M, Nader R, Al-Mefty O. Optic canal involvement in tuberculum sellae meningiomas: influence on approach, recurrence, and visual recovery. Neurosurgery. 2010;67(3)(Suppl Operative):ons108–ons119. - PubMed
-
- Nanda A, Ambekar S, Javalkar V, Sharma M. Technical nuances in the management of tuberculum sellae and diaphragma sellae meningiomas. Neurosurg Focus. 2013;35(6):E7. - PubMed
-
- Karsy M, Raheja A, Eli I, et al. Clinical outcomes with transcranial resection of the tuberculum sellae meningioma. World Neurosurg. 2017;108:748–755. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
