

Major Bleeding Predictors in Patients with Left Atrial Appendage Closure: The Iberian Registry II
- PMID: 32707736
- PMCID: PMC7408988
- DOI: 10.3390/jcm9072295
Major Bleeding Predictors in Patients with Left Atrial Appendage Closure: The Iberian Registry II
Abstract
Introduction and objective: Major bleeding events in patients undergoing left atrial appendage closure (LAAC) range from 2.2 to 10.3 per 100 patient-years in different series. This study aimed to clarify the bleeding predictive factors that could influence these differences.
Methods: LAAC was performed in 598 patients from the Iberian Registry II (1093 patient-years; median, 75.4 years). We conducted a multivariate analysis to identify predictive risk factors for major bleeding events. The occurrence of thromboembolic and bleeding events was compared to rates expected from CHA2DS2-VASc (congestive heart failure, hypertension, age, diabetes, stroke history, vascular disease, sex) and HAS-BLED (hypertension, abnormal renal and liver function, stroke, bleeding, labile INR, elderly, drugs or alcohol) scores.
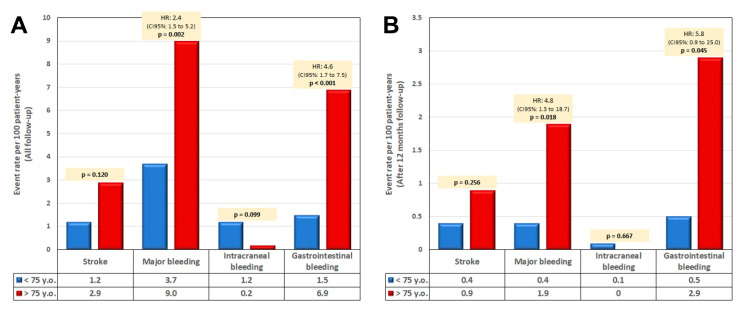
Results: Cox regression analysis revealed that age ≥75 years (HR: 2.5; 95% CI: 1.3 to 4.8; p = 0.004) and a history of gastrointestinal bleeding (GIB) (HR: 2.1; 95% CI: 1.1 to 3.9; p = 0.020) were two factors independently associated with major bleeding during follow-up. Patients aged <75 or ≥75 years had median CHA2DS2-VASc scores of 4 (IQR: 2) and 5 (IQR: 2), respectively (p < 0.001) and HAS-BLED scores were 3 (IQR: 1) and 3 (IQR: 1) for each group (p = 0.007). Events presented as follow-up adjusted rates according to age groups were stroke (1.2% vs. 2.9%; HR: 2.4, p = 0.12) and major bleeding (3.7 vs. 9.0 per 100 patient-years; HR: 2.4, p = 0.002). Expected major bleedings according to HAS-BLED scores were 6.2% vs. 6.6%, respectively. In patients with GIB history, major bleeding events were 6.1% patient-years (HAS-BLED score was 3.8 ± 1.1) compared to 2.7% patients-year in patients with no previous GIB history (HAS-BLED score was 3.4 ± 1.2; p = 0.029).
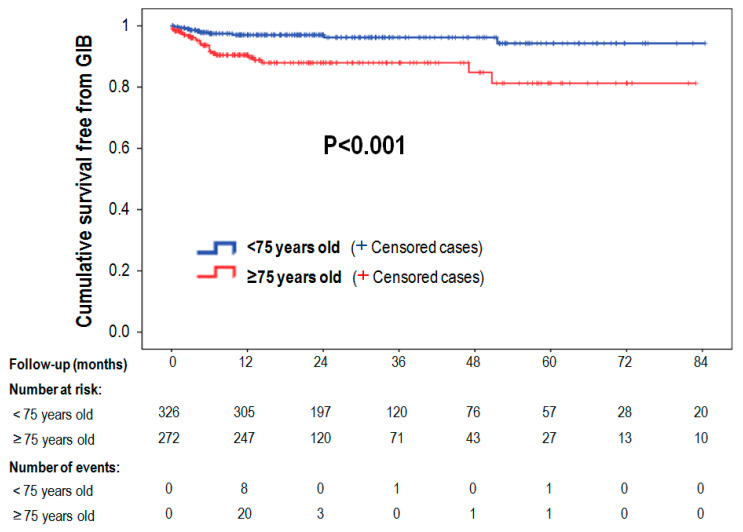
Conclusions: In this high-risk population, GIB history and age ≥75 years are the main predictors of major bleeding events after LAAC, especially during the first year. Age seems to have a greater influence on major bleeding events than on thromboembolic risk in these patients.
Keywords: age; atrial fibrillation; bleeding risk; left atrial appendage closure.
Conflict of interest statement
J.R. López-Mínguez, D. Arzamendi-Aizpurua, Ignacio Cruz and Xavi Freixa are proctors of Abbot for LAA closure with Amplatzer Cardiac Plug/Amulet; E. Infante De Oliveira, Ignacio Cruz-González and R. RuizSalmerón are proctors of Boston Scientific with Watchman device. Other authors declare no conflict of interest.
Figures
References
-
- Landmesser U., Tondo C., Camm J., Diener H.C., Paul V., Schmidt B., Settergren M., Teiger E., Nielsen-Kudsk J.E., Hildick-Smith D. Left atrial appendage occlusion with the AMPLATZER Amulet device: One-year follow-up from the prospective global Amulet observational registry. EuroIntervention. 2018;14:e590–e597. doi: 10.4244/EIJ-D-18-00344. - DOI - PubMed
-
- Phillips K.P., Santoso T., Sanders P., Alison J., Chan J.L.K., Pak H.N., Chandavimol M., Stein K.M., Gordon N., Razali O.B. Left atrial appendage closure with WATCHMAN in Asian patients: 2 year outcomes from the WASP registry. Int. J. Cardiol Heart Vasc. 2019;23:100358. doi: 10.1016/j.ijcha.2019.100358. - DOI - PMC - PubMed
-
- Freixa X., Gafoor S., Regueiro A., Cruz-Gonzalez I., Shakir S., Omran H., Berti S., Santoro G., Kefer J., Landmesser U., et al. Comparison of Efficacy and Safety of Left Atrial Appendage Occlusion in Patients Aged <75 to >/= 75 Years. Am. J. Cardiol. 2016;117:84–90. doi: 10.1016/j.amjcard.2015.10.024. - DOI - PubMed
-
- Lopez-Minguez J.R., Nogales-Asensio J.M., Infante De Oliveira E., De Gama Ribeiro V., Ruiz-Salmeron R., Arzamendi-Aizpurua D., Costa M., Gutierrez-Garcia H., Fernandez-Diaz J.A., Martin-Yuste V., et al. Long-term Event Reduction After Left Atrial Appendage Closure. Results of the Iberian Registry II. Rev. Esp. Cardiol. 2019;72:449–455. doi: 10.1016/j.rec.2018.03.017. - DOI - PubMed
LinkOut - more resources
Full Text Sources
