

Role of Cardiac Computed Tomography for Etiology Evaluation of Newly Diagnosed Heart Failure with Reduced Ejection Fraction
- PMID: 32708911
- PMCID: PMC7408702
- DOI: 10.3390/jcm9072270
Role of Cardiac Computed Tomography for Etiology Evaluation of Newly Diagnosed Heart Failure with Reduced Ejection Fraction
Abstract
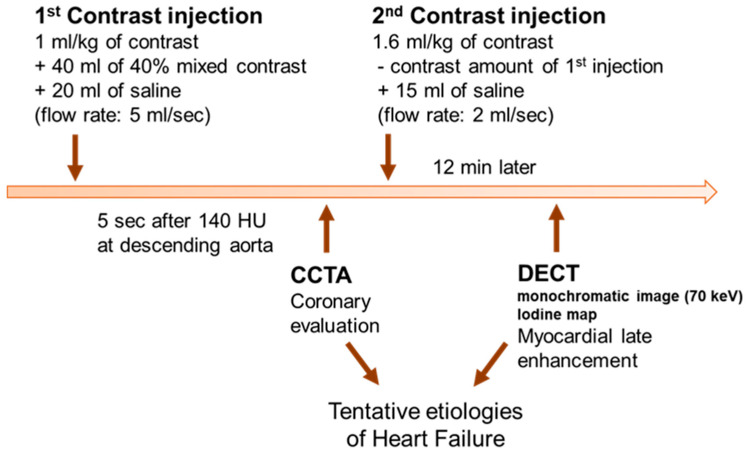
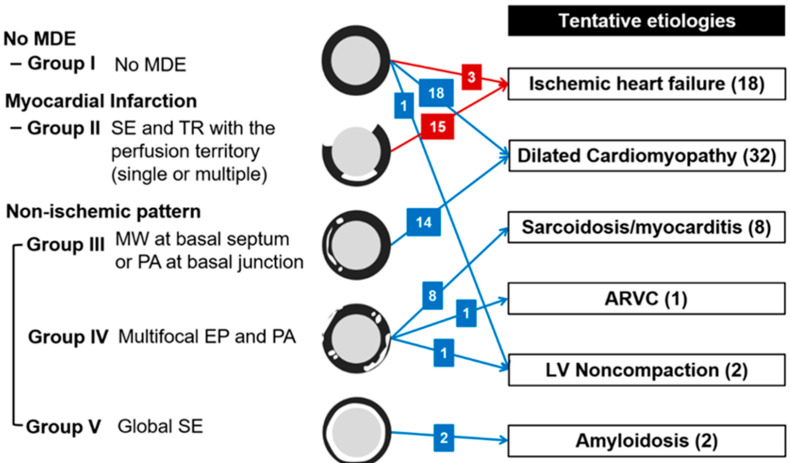
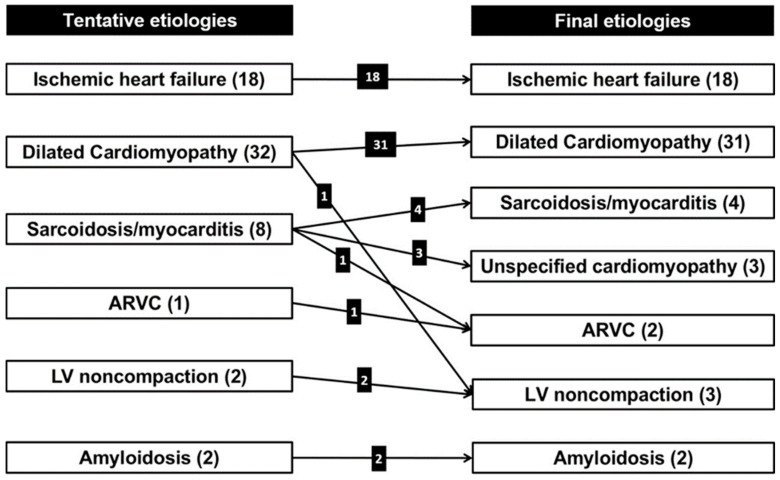
Delayed-enhanced dual-energy computed tomography (DECT) can evaluate the extent and degree of myocardial fibrosis while coronary CT angiography (CCTA) is a widely accepted coronary artery evaluation method. We sought to describe the role of combined cardiac CT for the evaluation of underlying etiology in patients with newly diagnosed heart failure with reduced ejection fraction (HFrEF). Sixty-three consecutive patients (31 men, 63 ± 16 years) with newly diagnosed HFrEF were enrolled in this prospective study. Coronary artery disease and myocardial fibrosis were evaluated on CCTA and DECT, respectively, and the tentative underlying etiologies of heart failure (HF) were determined with combinations of findings from both CTs. Concordance between tentative etiologies from cardiac CT and final etiologies from clinical decisions within a 2-year follow-up was assessed. Eighteen patients were diagnosed with ischemic HF on initial cardiac CT, and the final diagnosis was not changed. Another 45 patients with nonischemic HF included tentative etiologies of dilated cardiomyopathy (n = 32, 71.1%), sarcoidosis or myocarditis (n = 8, 17.8%), amyloidosis (n = 2, 4.4%), noncompaction (n = 2, 4.4%) and arrhythmogenic right ventricular cardiomyopathy (n = 1, 2.2%). Five nonischemic HF patients showed different etiologies between initial cardiac CT and clinical decisions. The concordance between cardiac CT and clinical decisions was 92.1%. A high degree of concordance was achieved between tentative etiologies from cardiac CT and final diagnoses from clinical decisions. Combined cardiac CT is a feasible, safe and effective imaging tool for the initial evaluation of newly diagnosed HFrEF patients.
Keywords: coronary computed tomographic angiography; delayed-enhanced cardiac computed tomography; etiology; heart failure with reduced ejection fraction.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ponikowski P., Voors A.A., Anker S.D., Bueno H., Cleland J.G.F., Coats A.J.S., Falk V., Gonzalez-Juanatey J.R., Harjola V.P., Jankowska E.A., et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the european society of cardiology (ESC)developed with the special contribution of the heart failure association (HFA) of the esc. Eur. Heart J. 2016;37:2129–2200. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
