

Evolution of therapies for the corneal endothelium: past, present and future approaches
- PMID: 32709756
- PMCID: PMC8005807
- DOI: 10.1136/bjophthalmol-2020-316149
Evolution of therapies for the corneal endothelium: past, present and future approaches
Erratum in
-
Correction: Evolution of therapies for the corneal endothelium: past, present and future approaches.Br J Ophthalmol. 2023 May;107(5):e1. doi: 10.1136/bjophthalmol-2020-316149.corr1. Br J Ophthalmol. 2023. PMID: 37080601 Free PMC article. No abstract available.
Abstract
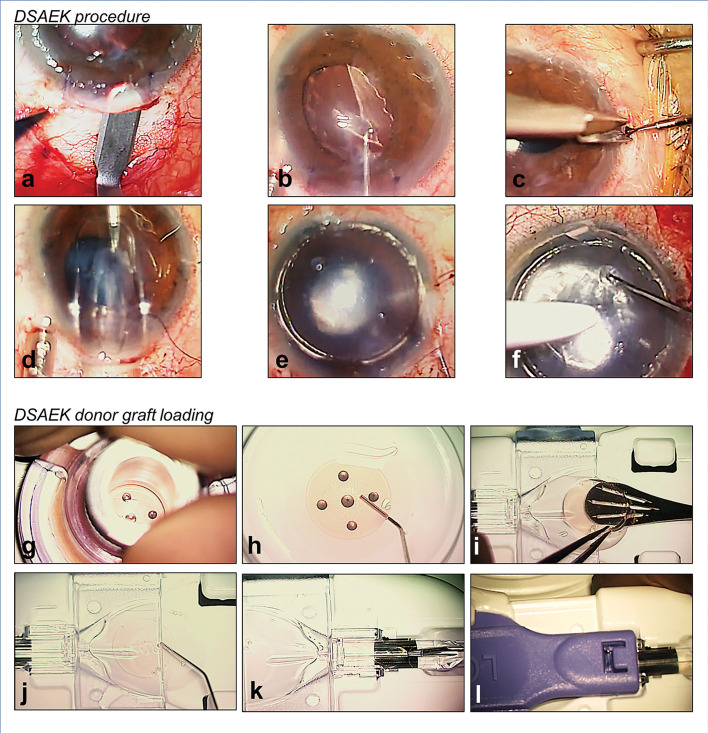
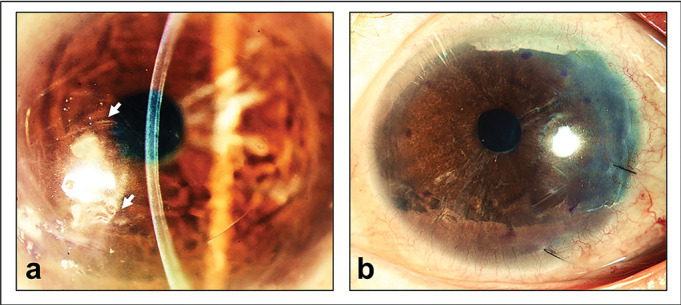
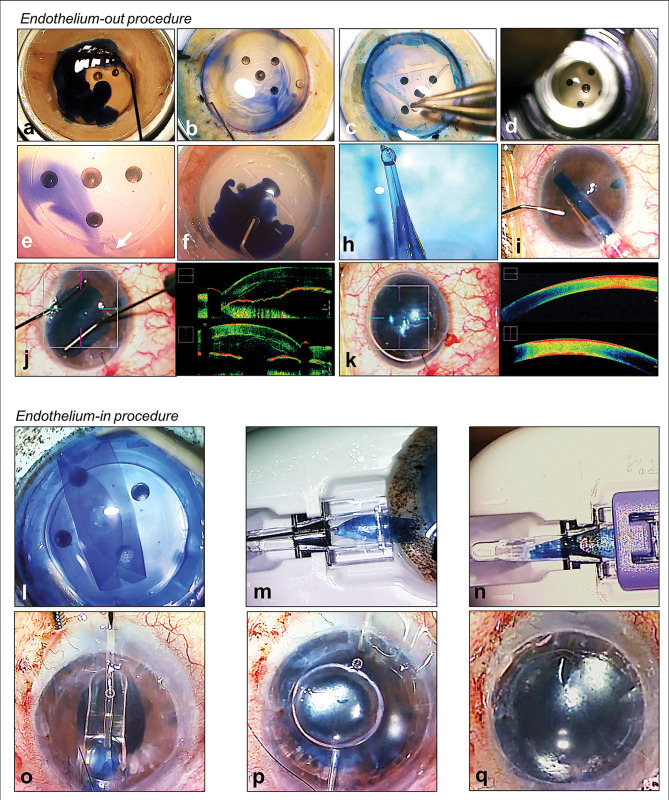
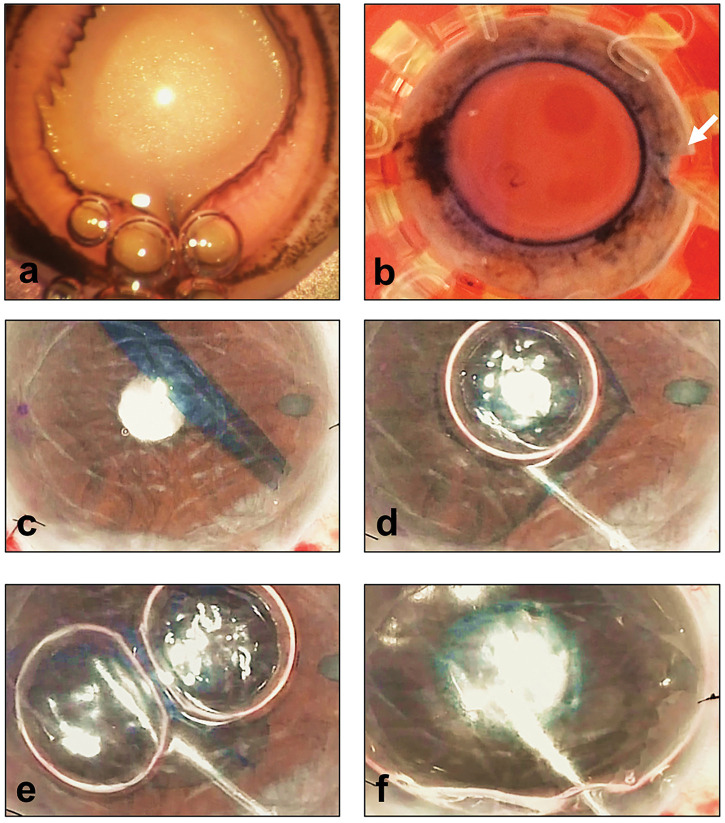
Corneal endothelial diseases are leading indications for corneal transplantations. With significant advancement in medical science and surgical techniques, corneal transplant surgeries are now increasingly effective at restoring vision in patients with corneal diseases. In the last 15 years, the introduction of endothelial keratoplasty (EK) procedures, where diseased corneal endothelium (CE) are selectively replaced, has significantly transformed the field of corneal transplantation. Compared to traditional penetrating keratoplasty, EK procedures, namely Descemet's stripping automated endothelial keratoplasty (DSAEK) and Descemet membrane endothelial keratoplasty (DMEK), offer faster visual recovery, lower immunological rejection rates, and improved graft survival. Although these modern techniques can achieve high success, there are fundamental impediments to conventional transplantations. A lack of suitable donor corneas worldwide restricts the number of transplants that can be performed. Other barriers include the need for specialized expertise, high cost, and risks of graft rejection or failure. Research is underway to develop alternative treatments for corneal endothelial diseases, which are less dependent on the availability of allogeneic tissues - regenerative medicine and cell-based therapies. In this review, an overview of past and present transplantation procedures used to treat corneal endothelial diseases are described. Potential novel therapies that may be translated into clinical practice will also be presented.
Keywords: Angiogenesis; Choroid; Fuchs’ endothelial dystrophy; Genetics; Imaging; Infection; Inflammation; Ocular surface; Stem Cells; Treatment Lasers; bullous keratopathy; cell therapy; cornea; corneal endothelium; corneal transplantation; eye (tissue) banking; keratoplasty; regenerative medicine.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JSM holds a patent on the EndoGlide and receive royalties. The other authors have no other relevant affiliations or financial involvement with any organisation or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
References
-
- Bahn CF, Glassman RM, MacCallum DK, et al. Postnatal development of corneal endothelium. Invest Ophthalmol Vis Sci 1986;27:44–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous