

Piperaquine resistant Cambodian Plasmodium falciparum clinical isolates: in vitro genotypic and phenotypic characterization
- PMID: 32711538
- PMCID: PMC7382038
- DOI: 10.1186/s12936-020-03339-w
Piperaquine resistant Cambodian Plasmodium falciparum clinical isolates: in vitro genotypic and phenotypic characterization
Abstract
Background: High rates of dihydroartemisinin-piperaquine (DHA-PPQ) treatment failures have been documented for uncomplicated Plasmodium falciparum in Cambodia. The genetic markers plasmepsin 2 (pfpm2), exonuclease (pfexo) and chloroquine resistance transporter (pfcrt) genes are associated with PPQ resistance and are used for monitoring the prevalence of drug resistance and guiding malaria drug treatment policy.
Methods: To examine the relative contribution of each marker to PPQ resistance, in vitro culture and the PPQ survival assay were performed on seventeen P. falciparum isolates from northern Cambodia, and the presence of E415G-Exo and pfcrt mutations (T93S, H97Y, F145I, I218F, M343L, C350R, and G353V) as well as pfpm2 copy number polymorphisms were determined. Parasites were then cloned by limiting dilution and the cloned parasites were tested for drug susceptibility. Isobolographic analysis of several drug combinations for standard clones and newly cloned P. falciparum Cambodian isolates was also determined.
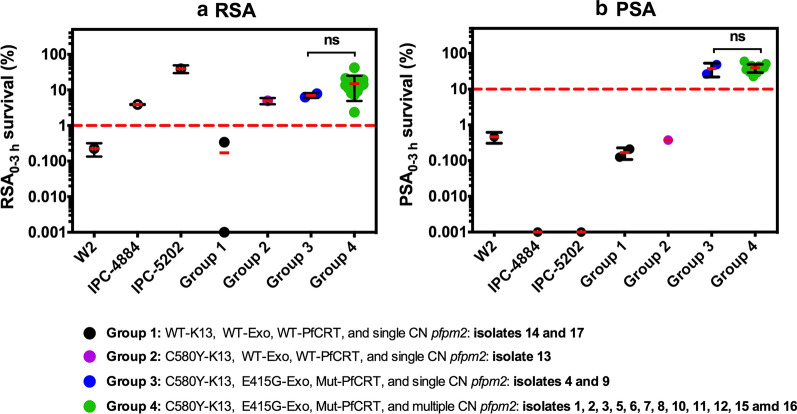
Results: The characterization of culture-adapted isolates revealed that the presence of novel pfcrt mutations (T93S, H97Y, F145I, and I218F) with E415G-Exo mutation can confer PPQ-resistance, in the absence of pfpm2 amplification. In vitro testing of PPQ resistant parasites demonstrated a bimodal dose-response, the existence of a swollen digestive vacuole phenotype, and an increased susceptibility to quinine, chloroquine, mefloquine and lumefantrine. To further characterize drug sensitivity, parental parasites were cloned in which a clonal line, 14-B5, was identified as sensitive to artemisinin and piperaquine, but resistant to chloroquine. Assessment of the clone against a panel of drug combinations revealed antagonistic activity for six different drug combinations. However, mefloquine-proguanil and atovaquone-proguanil combinations revealed synergistic antimalarial activity.
Conclusions: Surveillance for PPQ resistance in regions relying on DHA-PPQ as the first-line treatment is dependent on the monitoring of molecular markers of drug resistance. P. falciparum harbouring novel pfcrt mutations with E415G-exo mutations displayed PPQ resistant phenotype. The presence of pfpm2 amplification was not required to render parasites PPQ resistant suggesting that the increase in pfpm2 copy number alone is not the sole modulator of PPQ resistance. Genetic background of circulating field isolates appear to play a role in drug susceptibility and biological responses induced by drug combinations. The use of latest field isolates may be necessary for assessment of relevant drug combinations against P. falciparum strains and when down-selecting novel drug candidates.
Keywords: Drug combination; Exonuclease; Malaria; PfCRT; Piperaquine resistance; Plasmepsin.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- WHO . World malaria report. Geneva: World Health Organization; 2019.
-
- WHO . Guidelines fro the treatment of malaria. 3. Geneva: World Health Organization Press; 2015. - PubMed
-
- Saunders DL, Vanachayangkul P, Lon C, Program USAMMR, National Center for Parasitology, Entomology, Malaria Control, Royal Cambodian Armed Forces Dihydroartemisinin–piperaquine failure in Cambodia. N Engl J Med. 2014;371:484–485. - PubMed
-
- Leang R, Taylor WR, Bouth DM, Song L, Tarning J, Char MC, et al. Evidence of Plasmodium falciparum malaria multidrug resistance to artemisinin and piperaquine in Western Cambodia: dihydroartemisinin-piperaquine open-label multicenter clinical assessment. Antimicrob Agents Chemother. 2015;59:4719–4726. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
