

Accuracy of time to treatment estimates in the CRASH-3 clinical trial: impact on the trial results
- PMID: 32711551
- PMCID: PMC7382791
- DOI: 10.1186/s13063-020-04623-5
Accuracy of time to treatment estimates in the CRASH-3 clinical trial: impact on the trial results
Abstract
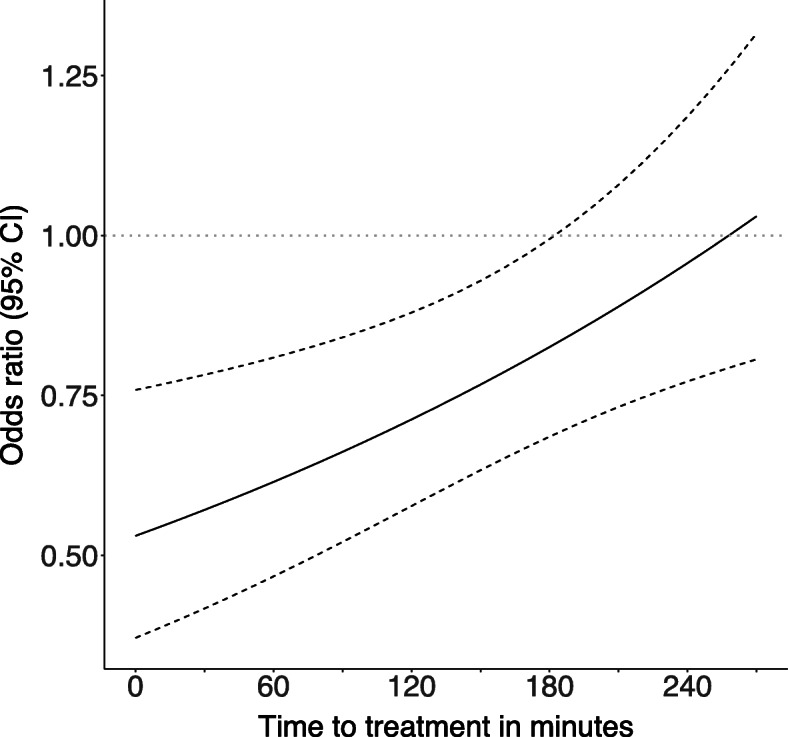
Background: Early treatment with tranexamic acid may reduce deaths after traumatic brain injury (TBI). In mild and moderate TBI, there is a time to treatment interaction, with early treatment being most beneficial. Time to treatment was recorded by clinicians and is subject to error. Using monitoring data from the CRASH-3 trial, we examine the impact of errors in time to treatment on estimated treatment effects.
Methods: The CRASH-3 trial was a randomised trial of the effect of tranexamic acid on death and vascular occlusive events in 12,737 TBI patients. This analysis includes the 8107 patients with a Glasgow coma scale score of 9 to 15 since previous analyses showed that these patients benefit most from early treatment. Clinician-recorded time to treatment was checked against ambulance and hospital records for 1368/12,737 (11%) patients. Patients who died were preferentially selected for monitoring and we monitored 36% of head injury deaths. We describe measurement errors using Bland-Altman graphs. We model the effect of tranexamic acid on head injury death using logistic regression with a time-treatment interaction term. We use regression calibration, multiple imputation and Bayesian analysis to estimate the impact of time to treatment errors.
Results: Clinicians rounded times to the nearest half or full hour in 66% of cases. Monitored times were also rounded and were identical to clinician times in 63% of patients. Times were underestimated by an average of 9 min (95% CI - 85, 66). There was more variability between clinician-recorded and monitored times in low- and middle-income countries than in high-income countries. The treatment effect estimate at 1 h was greater for monitored times OR = 0.61 (95% CI 0.47, 0.81) than for clinician-recorded times OR = 0.63 (95% CI 0.48, 0.83). All three adjustment methods gave similar time to treatment interactions. For Bayesian methods, the treatment effect at 1 h was OR = 0.58 (95% CI 0.43, 0.78). Using monitored times increased the time-treatment interaction term from 1.15 (95% CI 1.03, 1.27) to 1.16 (95% CI 1.05, 1.28).
Conclusions: Accurate estimation of time from injury to treatment is challenging, particularly in low resource settings. Adjustment for known errors in time to treatment had minimal impact on the trial results.
Trial registration: ClinicalTrials.gov NCT01402882 . Registered on 25 July 2011.
Keywords: Antifibrinolytic; Monitoring; Tranexamic acid; Traumatic brain injury; measurement error.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- CRASH-2 trial collaborators. Shakur H, Roberts I, Bautista R, Caballero J, Coats T, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH- 2): a randomised, placebo-controlled trial. Lancet. 2010;376:23–32. doi: 10.1016/S0140-6736(10)60835-5. - DOI - PubMed
-
- Adeyemi B, Dallaku K, Idris H, Wangui R, Gul J, Jabeen K, et al. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet. 2017;389(10084):2105–2116. doi: 10.1016/S0140-6736(17)30638-4. - DOI - PMC - PubMed
-
- Gayet-Ageron A, Prieto-Merino D, Ker K, Shakur H, Ageron FX, Roberts I, et al. Effect of treatment delay on the effectiveness and safety of antifibrinolytics in acute severe haemorrhage: a meta-analysis of individual patient-level data from 40138 bleeding patients. Lancet. 2018;391(10116):125–132. doi: 10.1016/S0140-6736(17)32455-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
