

Multiple MitraClips: The balancing act between pressure gradient and regurgitation
- PMID: 32711989
- PMCID: PMC7704541
- DOI: 10.1016/j.jtcvs.2020.05.049
Multiple MitraClips: The balancing act between pressure gradient and regurgitation
Abstract
Objective: Transcatheter mitral valve repair with the MitraClip is used for the symptomatic management of mitral regurgitation (MR). The challenge is reducing MR while avoiding an elevated mitral valve gradient (MVG). This study assesses how multiple MitraClips used to treat MR can affect valve performance.
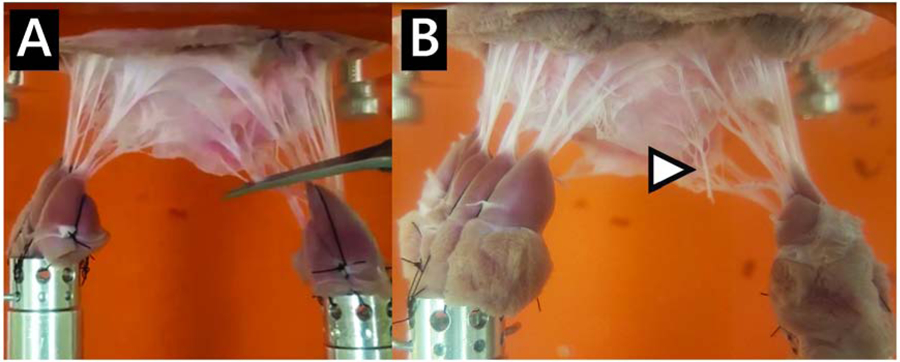
Methods: Six porcine mitral valves were assessed using an in vitro left heart simulator in the native, moderate-to-severe MR, and severe MR cases. MR cases were tested in the no-MitraClip, 1-MitraClip, and 2-MitraClip configurations. Mitral regurgitant fraction (MRF), MVG, and effective orifice area (EOA) were quantified.
Results: Native MRF, MVG, and EOA were 14.22%, 2.59 mm Hg, and 1.64 cm2, respectively. For moderate-to-severe MR, MRF, MVG, and EOA were 34.07%, 3.31 mm Hg, and 2.22 cm2, respectively. Compared with the no-MitraClip case, 1 MitraClip decreased MRF to 18.57% (P < .0001) and EOA to 1.50 cm2 (P = .0002). MVG remained statistically unchanged (3.44 mm Hg). Two MitraClips decreased MRF to 14.26% (P < .0001) and EOA to 1.36 cm2 (P = .0001). MVG remained unchanged (3.29 mm Hg). For severe MR, MRF, MVG, and EOA were 59.79%, 4.98 mm Hg, and 2.73 cm2, respectively. Compared with the no-MitraClip case, 1 MitraClip decreased MRF to 30.72% (P < .0001) and EOA to 1.82 cm2 (P < .0001); MVG remained unchanged (4.03 mm Hg). MVG remained statistically unchanged. Two MitraClips decreased MRF to 23.10% (P < .0001) and EOA to 1.58 cm2 (P < .0001); MVG remained statistically unchanged (3.82 mm Hg). Both MR models yielded no statistical difference between 1 and 2 MitraClips.
Conclusions: There is limited concern regarding elevation of MVG when reducing MR using 1 or 2 MitraClips, although 2 MitraClips did not significantly continue to reduce MRF.
Keywords: MitraClip; PIV; double orifice; mitral regurgitation; mitral valve; ventricular flow.
Copyright © 2020 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: L.P. Dasi reports having patent applications filed on novel polymeric valves, vortex generators and superhydrophobic/omniphobic surfaces. The other authors report no conflicts.
Figures







Comment in
-
Commentary: Between Scylla and Charybdis.J Thorac Cardiovasc Surg. 2022 Apr;163(4):1331-1332. doi: 10.1016/j.jtcvs.2020.06.031. Epub 2020 Jun 27. J Thorac Cardiovasc Surg. 2022. PMID: 32680637 No abstract available.
-
Commentary: The importance of annulus in percutaneous mitral valve repair.J Thorac Cardiovasc Surg. 2022 Apr;163(4):1329-1330. doi: 10.1016/j.jtcvs.2020.06.056. Epub 2020 Jun 28. J Thorac Cardiovasc Surg. 2022. PMID: 32711993 No abstract available.
-
Commentary: The good, the bad, and the ugly.J Thorac Cardiovasc Surg. 2022 Apr;163(4):1328-1329. doi: 10.1016/j.jtcvs.2020.06.104. Epub 2020 Jul 13. J Thorac Cardiovasc Surg. 2022. PMID: 32807559 No abstract available.
References
-
- Benjamin EJ, et al., Heart disease and stroke statistics—2018 update: a report from the American Heart Association. Circulation, 2018. 137(12): p. e67–e492. - PubMed
-
- Boudoulas KD, et al., Factors determining left atrial kinetic energy in patients with chronic mitral valve disease. Herz, 2003. 28(5): p. 437–444. - PubMed
-
- Aspirus Heart & Vascular Institute. TMVR - Mitral Valve Repair. 2013. [cited 2020; Available from: https://www.valvedisease.org/index.cfm?pid=23&pageTitle=TMVR---Mitral-Va....
-
- Obadia J-F, et al., Percutaneous repair or medical treatment for secondary mitral regurgitation. New England Journal of Medicine, 2018. 379(24): p. 2297–2306. - PubMed
-
- Stone GW, et al., Transcatheter mitral-valve repair in patients with heart failure. New England Journal of Medicine, 2018. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
