

Stratifying chronic stroke patients based on the influence of contralesional motor cortices: An inter-hemispheric inhibition study
- PMID: 32712080
- PMCID: PMC7487004
- DOI: 10.1016/j.clinph.2020.06.016
Stratifying chronic stroke patients based on the influence of contralesional motor cortices: An inter-hemispheric inhibition study
Abstract
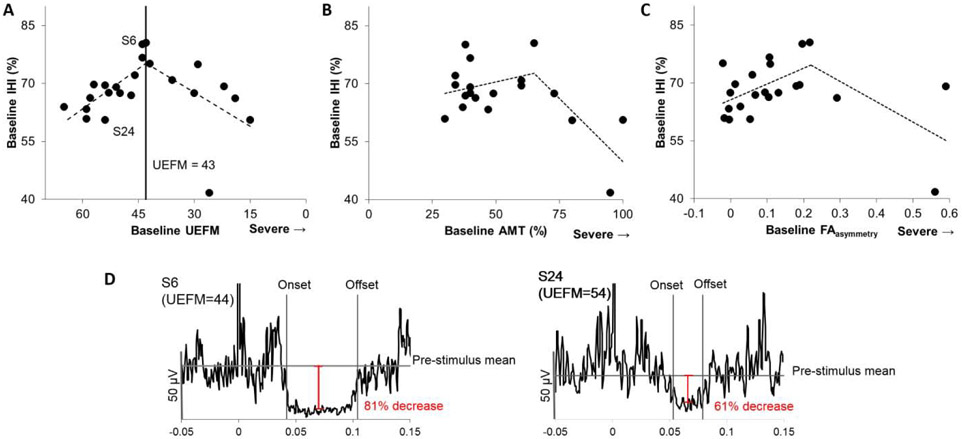
Objective: A recent "bimodal-balance recovery" model suggests that contralesional influence varies based on the amount of ipsilesional reserve: inhibitory when there is a large reserve, but supportive when there is a low reserve. Here, we investigated the relationships between contralesional influence (inter-hemispheric inhibition, IHI) and ipsilesional reserve (corticospinal damage/impairment), and also defined a criterion separating subgroups based on the relationships.
Methods: Twenty-four patients underwent assessment of IHI using Transcranial Magnetic Stimulation (ipsilateral silent period method), motor impairment using Upper Extremity Fugl-Meyer (UEFM), and corticospinal damage using Diffusion Tensor Imaging and active motor threshold. Assessments of UEFM and IHI were repeated after 5-week rehabilitation (n = 21).
Results: Relationship between IHI and baseline UEFM was quadratic with criterion at UEFM 43 (95%conference interval: 40-46). Patients less impaired than UEFM = 43 showed stronger IHI with more impairment, whereas patients more impaired than UEFM = 43 showed lower IHI with more impairment. Of those made clinically-meaningful functional gains in rehabilitation (n = 14), more-impaired patients showed further IHI reduction.
Conclusions: A criterion impairment-level can be derived to stratify patient-subgroups based on the bimodal influence of contralesional cortex. Contralesional influence also evolves differently across subgroups following rehabilitation.
Significance: The criterion may be used to stratify patients to design targeted, precision treatments.
Keywords: Corticospinal; Diffusion Tensor Imaging (DTI); Inter-Hemispheric Inhibition (IHI); Motor function; Rehabilitation; Stroke; Transcranial Magnetic Stimulation (TMS); Upper limb.
Copyright © 2020 International Federation of Clinical Neurophysiology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest Andre G. Machado has the following conflicts of interest: ATI, Enspire and Cardionomics (distribution rights from intellectual property), St Jude (consultant) and Medtronic (Fellowship support). Other authors declare that there is no conflict of interest associated with this work. Specifically, there are no financial or personal relationships with other people or organizations that could inappropriately influence or bias this work.
Figures


Comment in
-
The balance recovery bimodal model in stroke patients between evidence and speculation: Do recent studies support it?Clin Neurophysiol. 2020 Oct;131(10):2488-2490. doi: 10.1016/j.clinph.2020.07.004. Epub 2020 Jul 22. Clin Neurophysiol. 2020. PMID: 32747189 No abstract available.
-
On the issue of measuring interhemispheric inhibition in unilateral stroke.Clin Neurophysiol. 2021 Feb;132(2):688-689. doi: 10.1016/j.clinph.2020.09.028. Epub 2020 Oct 29. Clin Neurophysiol. 2021. PMID: 33172778 No abstract available.
-
Reply to "On the issue of measuring interhemispheric inhibition in unilateral stroke".Clin Neurophysiol. 2021 Feb;132(2):690-691. doi: 10.1016/j.clinph.2020.10.004. Epub 2020 Oct 29. Clin Neurophysiol. 2021. PMID: 33288405 No abstract available.
References
-
- Berglund K, Fugl-Meyer AR. Upper extremity function in hemiplegia. A cross-validation study of two assessment methods. Scand J Rehabil Med 1986;18(4):155–7. - PubMed
-
- Boddington LJ, Reynolds JN. Targeting interhemispheric inhibition with neuromodulation to enhance stroke rehabilitation. Brain Stimul 2017;10(2):214–22. - PubMed
-
- Boroojerdi B, Diefenbach K, Ferbert A. Transcallosal inhibition in cortical and subcortical cerebral vascular lesions. J Neurol Sci 1996;144(1-2):160–70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
