

COVID-19: immunopathogenesis and Immunotherapeutics
- PMID: 32712629
- PMCID: PMC7381863
- DOI: 10.1038/s41392-020-00243-2
COVID-19: immunopathogenesis and Immunotherapeutics
Abstract
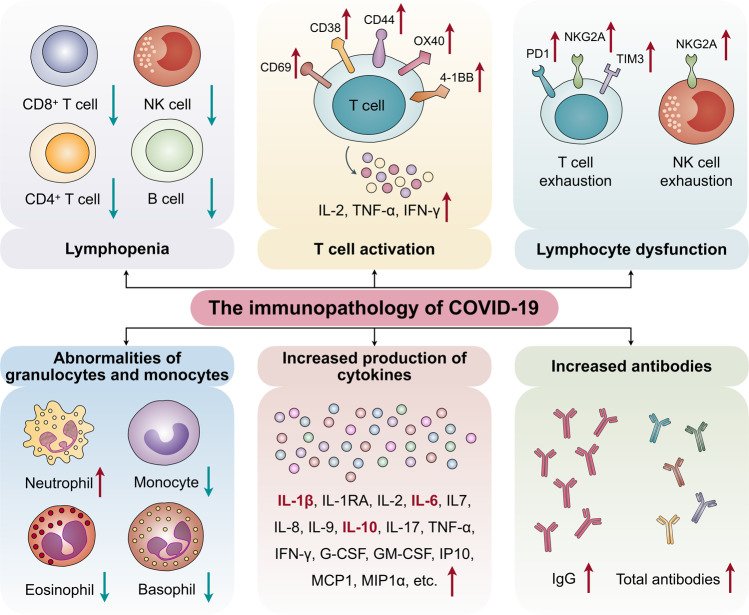
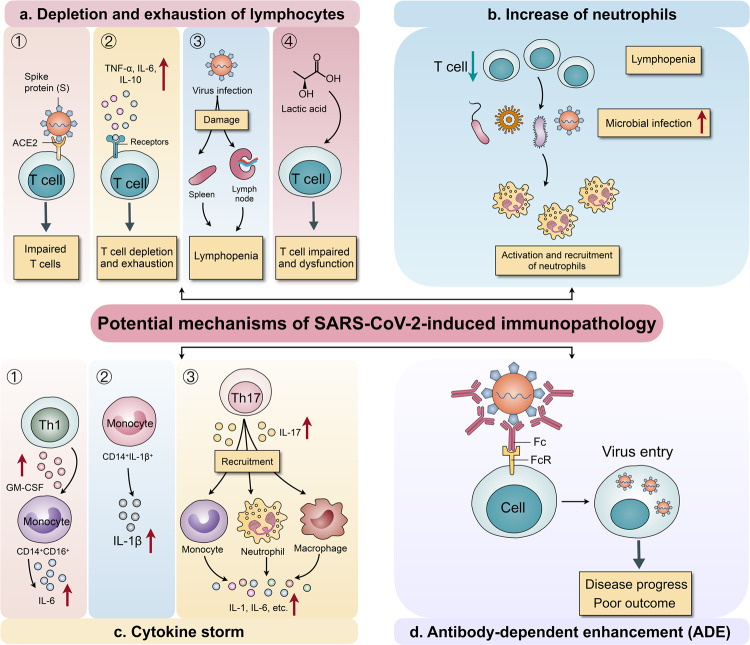
The recent novel coronavirus disease (COVID-19) outbreak, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is seeing a rapid increase in infected patients worldwide. The host immune response to SARS-CoV-2 appears to play a critical role in disease pathogenesis and clinical manifestations. SARS-CoV-2 not only activates antiviral immune responses, but can also cause uncontrolled inflammatory responses characterized by marked pro-inflammatory cytokine release in patients with severe COVID-19, leading to lymphopenia, lymphocyte dysfunction, and granulocyte and monocyte abnormalities. These SARS-CoV-2-induced immune abnormalities may lead to infections by microorganisms, septic shock, and severe multiple organ dysfunction. Therefore, mechanisms underlying immune abnormalities in patients with COVID-19 must be elucidated to guide clinical management of the disease. Moreover, rational management of the immune responses to SARS-CoV-2, which includes enhancing anti-viral immunity while inhibiting systemic inflammation, may be key to successful treatment. In this review, we discuss the immunopathology of COVID-19, its potential mechanisms, and clinical implications to aid the development of new therapeutic strategies against COVID-19.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
