

Cost-effectiveness of Preemptive Therapy Versus Prophylaxis in a Randomized Clinical Trial for the Prevention of Cytomegalovirus Disease in Seronegative Liver Transplant Recipients With Seropositive Donors
- PMID: 32712663
- PMCID: PMC8563196
- DOI: 10.1093/cid/ciaa1051
Cost-effectiveness of Preemptive Therapy Versus Prophylaxis in a Randomized Clinical Trial for the Prevention of Cytomegalovirus Disease in Seronegative Liver Transplant Recipients With Seropositive Donors
Abstract
Background: The relative costs of preemptive therapy (PET) or prophylaxis for the prevention of cytomegalovirus (CMV) disease in high-risk donor CMV-seropositive/recipient-seronegative (D+/R-) liver transplant recipients have not been assessed in the context of a randomized trial.
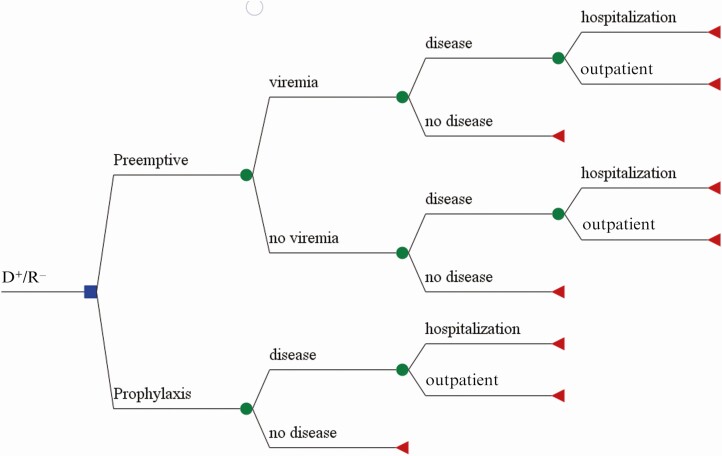
Methods: A decision tree model was constructed based on the probability of outcomes in a randomized controlled trial that compared valganciclovir as PET or prophylaxis for 100 days in 205 D+/R- liver transplant recipients. Itemized costs for each site were obtained from a federal cost transparency database. Total costs included costs of implementation of the strategy and CMV disease treatment-related costs. Net cost per patient was estimated from the decision tree for each strategy.
Results: PET was associated with a 10% lower absolute rate of CMV disease (9% vs 19%). The cost of treating a case of CMV disease in our patients was $88 190. Considering cost of implementation of strategy and treatment-related cost for CMV disease, the net cost-savings per patient associated with PET was $8707 compared to prophylaxis. PET remained cost-effective across a range of assumptions (varying costs of monitoring and treatment, and rates of disease).
Conclusions: PET is the dominant CMV prevention strategy in that it was associated with lower rates of CMV disease and lower overall costs compared to prophylaxis in D+/R- liver transplant recipients. Costs were driven primarily by more hospitalizations and higher CMV disease-associated costs due to delayed onset postprophylaxis disease in the prophylaxis group.
Keywords: cytomegalovirus; CMV; cost-effectiveness; preemptive therapy; transplant.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Ho M. The history of cytomegalovirus and its diseases. Med Microbiol Immunol 2008; 197:65–73. - PubMed
-
- Lumbreras C, Manuel O, Len O, ten Berge IJ, Sgarabotto D, Hirsch HH. Cytomegalovirus infection in solid organ transplant recipients. Clin Microbiol Infect 2014; 20:19–26. - PubMed
-
- Ljungman P, Boeckh M, Hirsch HH, et al. Disease Definitions Working Group of the Cytomegalovirus Drug Development Forum . Definitions of cytomegalovirus infection and disease in transplant patients for use in clinical trials. Clin Infect Dis 2017; 64:87–91. - PubMed
-
- Falagas ME, Arbo M, Ruthazer R, et al. Cytomegalovirus disease is associated with increased cost and hospital length of stay among orthotopic liver transplant recipients. Transplantation 1997; 63:1595–601. - PubMed
-
- Kim WR, Badley AD, Wiesner RH, et al. The economic impact of cytomegalovirus infection after liver transplantation. Transplantation 2000; 69:357–61. - PubMed
