

Kimura Disease Presenting with Buccal Mass: A Case Report and Literature Review
- PMID: 32712881
- PMCID: PMC8134605
- DOI: 10.1007/s12105-020-01206-3
Kimura Disease Presenting with Buccal Mass: A Case Report and Literature Review
Abstract
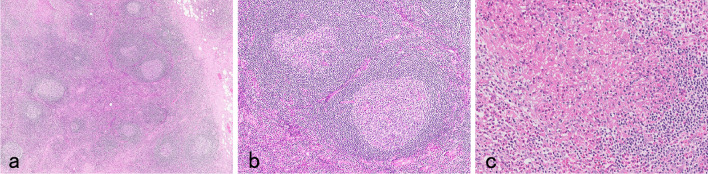
A 52-year-old man with a 2-year history of left buccal swelling was admitted to our department. An elastic hard oral mass was palpated under the intact buccal mucosa. A CT scan with enhancement revealed a solid mass measuring 2.0 × 1.5 × 1.3 cm between the left masseter muscle and the maxilla. Laboratory examination showed elevated peripheral blood eosinophil count of 1070/μL (12.3%) and serum immunoglobulin (Ig)E level of 1374 IU/mL. Histologic examination of transorally excised mass revealed lymphoid follicular hyperplasia with reactive germinal centers and eosinophilic infiltration with eosinophilic micro-abscesses in the germinal centers. Abundant IgE deposition in a reticular fashion was observed in the germinal centers and c-kit positive mast cells was observed in the paracortical area in the excised mass. The patient was diagnosed with Kimura disease (KD) and treated with oral prednisolone, tapering from 10 mg/day for approximately 8 months. Eosinophil count and serum IgE level decreased to 435/μL (5%) and 520 IU/dL, respectively. He is free from symptoms at the time of this submission. KD, a rare, benign, and chronic inflammatory disorder, occurs predominantly in young male adults in Asia. Patients with KD who presents with buccal mass are relatively rare. Immunohistologic analyses suggested that an allergic reaction played an important role in the etiology of KD in this case.
Keywords: Buccal mass; Eosinophil; Immunoglobulin E; Kimura disease; Steroid.
Conflict of interest statement
The authors declare that there are no actual or potential conflicts of interest in relation to this article.
Figures




References
-
- Kimura T, Yoshimura S, Ishikawa H. Unusual granuration combained with hyperplastic change of lymphoid tissues. Trans Soc Pathol Jpn. 1948;37:179–180.
-
- Ishii M. Kimura disease (in Japanease) ORL Tokyo. 1982;25(4):407–416.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
