

Hamburger Technique: Augmented Rotator Cuff Repair With Biological Superior Capsular Reconstruction
- PMID: 32714809
- PMCID: PMC7372565
- DOI: 10.1016/j.eats.2020.03.022
Hamburger Technique: Augmented Rotator Cuff Repair With Biological Superior Capsular Reconstruction
Abstract
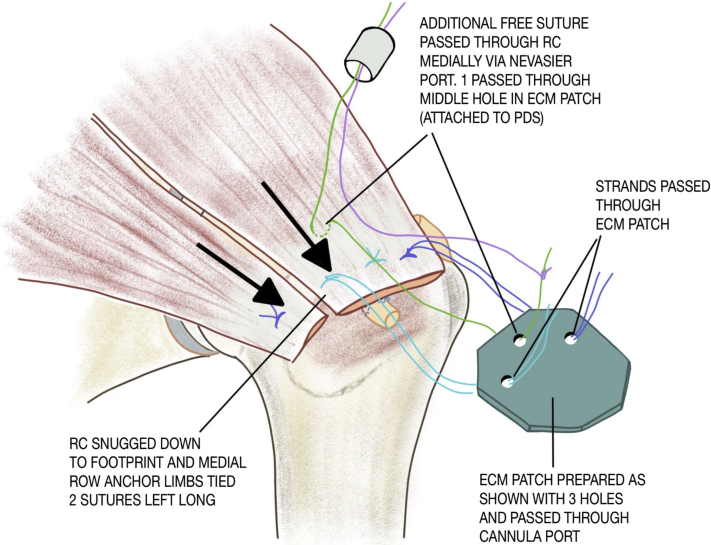
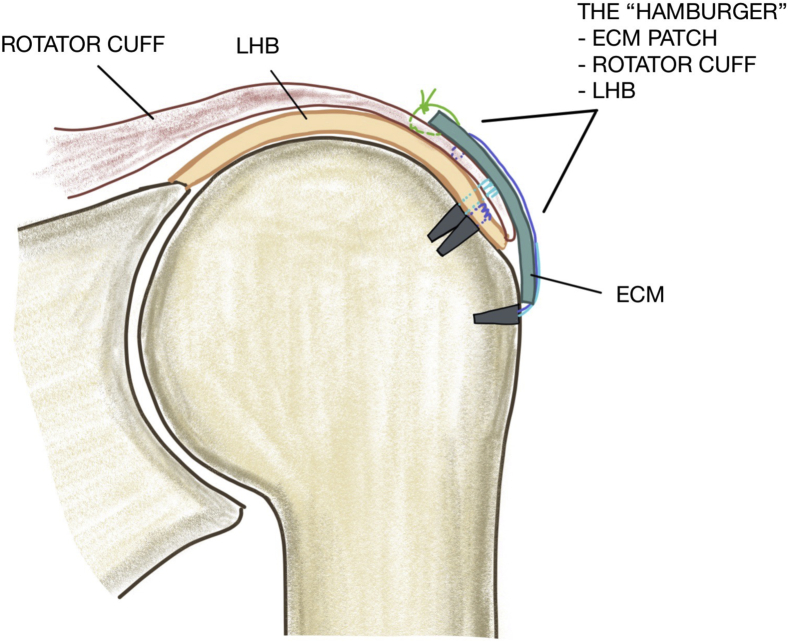
Despite profound advancements in arthroscopic rotator cuff repair (RCR) techniques, radiologic failure rates may be in excess of 60% with repairs of large and massive tears in the elderly population. One of the strategies to improve these healing rates has been "patch" augmentation of the cuff repair. At the same time, superior capsular reconstruction (SCR) has gained significant popularity as an option for irreparable rotator cuff (RC) tears. Some have also advocated performing SCR in addition to arthroscopic RCR to reinforce the repair and improve healing rates. Techniques involving the use of fascia lata, ECM patches, and long head of the biceps (LHB) for SCR to reinforce the cuff repair have all been elegantly described. In this article, we propose a technique that enables a combination of the aforementioned procedures and involves performing RCR with patch augmentation, as well as SCR using LHB. In doing so, the repaired RC is bordered by the patch over its bursal surface and the LHB on the articular surface (functioning as the superior capsule), thus giving us the name "Hamburger technique" (a 3-layered construct).
© 2020 by the Arthroscopy Association of North America. Published by Elsevier.
Figures





References
-
- Mihata T., Lee T.Q., Watanabe C. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy. 2013;29:459–470. - PubMed
LinkOut - more resources
Full Text Sources
