

Management of Orthostatic Hypotension in Parkinson's Disease
- PMID: 32716319
- PMCID: PMC7592655
- DOI: 10.3233/JPD-202036
Management of Orthostatic Hypotension in Parkinson's Disease
Abstract
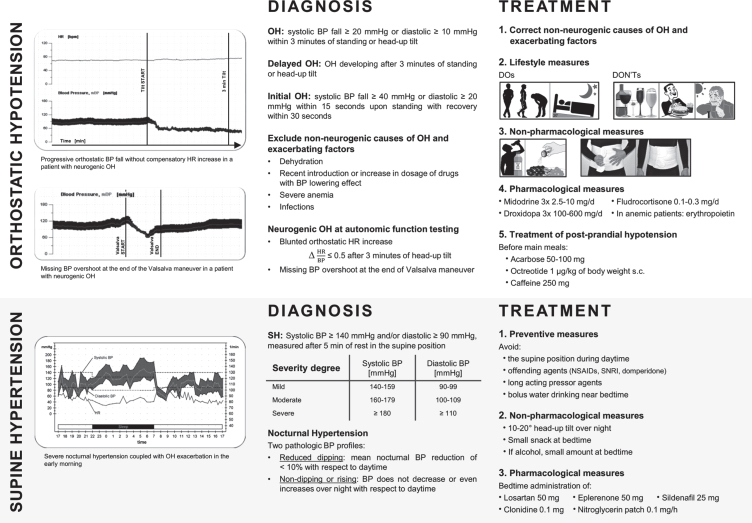
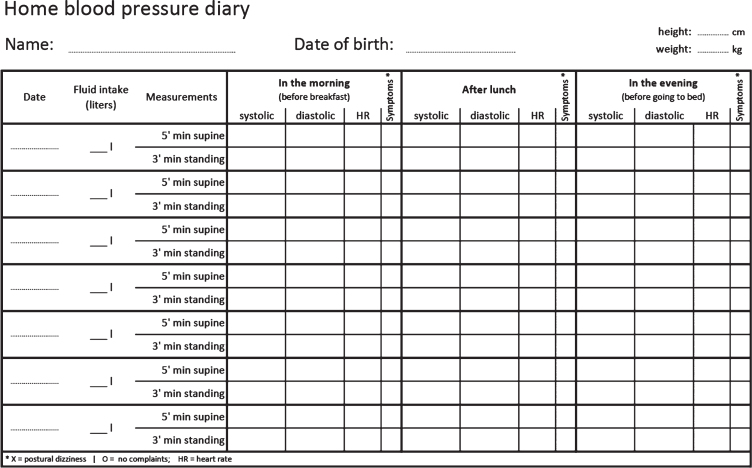
Orthostatic hypotension (OH) is a common non-motor feature of Parkinson's disease that may cause unexplained falls, syncope, lightheadedness, cognitive impairment, dyspnea, fatigue, blurred vision, shoulder, neck, or low-back pain upon standing. Blood pressure (BP) measurements supine and after 3 minutes upon standing screen for OH at bedside. The medical history and cardiovascular autonomic function tests ultimately distinguish neurogenic OH, which is due to impaired sympathetic nerve activity, from non-neurogenic causes of OH, such as hypovolemia and BP lowering drugs. The correction of non-neurogenic causes and exacerbating factors, lifestyle changes and non-pharmacological measures are the cornerstone of OH treatment. If these measures fail, pharmacological interventions (sympathomimetic agents and/or fludrocortisone) should be introduced stepwise depending on the severity of symptoms. About 50% of patients with neurogenic OH also suffer from supine and nocturnal hypertension, which should be monitored for with in-office, home and 24 h-ambulatory BP measurements. Behavioral measures help prevent supine hypertension, which is eventually treated with non-pharmacological measures and bedtime administration of short-acting anti-hypertensive drugs in severe cases. If left untreated, OH impacts on activity of daily living and increases the risk of syncope and falls. Supine hypertension is asymptomatic, but often limits an effective treatment of OH, increases the risk of hypertensive emergencies and, combined with OH, facilitates end-organ damage. A timely management of both OH and supine hypertension ameliorates quality of life and prevents short and long-term complications in patients with Parkinson's disease.
Keywords: Parkinson’s disease; nocturnal hypertension; orthostatic hypotension; post-prandial hypotension; supine hypertension.
Conflict of interest statement
Full financial disclosures for the last 12 months
Alessandra Fanciulli: Dr. Fanciulli reports royalties from Springer Nature Publishing Group, speaker fees and honoraria from the Austrian Autonomic Society, Austrian Parkinson Society, Ordensklinikum Linz, International Parkinson Disease and Movement Disorders Society and Theravance Biopharma and research grants from the Stichting ParkinsonFond and the Österreichischer Austausch Dienst, outside of the submitted work.
Fabian Leys: Dr. Leys reports no disclosures.
Cristian Falup-Pecurariu: Dr. Falup-Pecurariu reports royalties from Springer Nature Publishing Group, speaker fees and honoraria from the International Parkinson and Movement Disorders Society, outside of the submitted work.
Roland Thijs: Dr. Thijs reports speaker fees from Novartis, consultancy fees from Theravance Biopharma and research support from the Dutch Epilepsy Foundation Dutch, the Netherlands Organization for Health Research and Development (ZonMW) and De Christelijke Vereniging voor de Verpleging van Lijders aan Epilepsie, outside of the submitted work.
Gregor K. Wenning: Dr. Wenning reports consultancy fees from Biogen, Biohaven, Lundbeck, Minoryx, Takeda, Theravance and research support from the Austrian Science Fund, International Parkinson Disease and Movement Disorders Society and the Medical University Innsbruck, outside of the submitted work.
Figures
References
-
- Milazzo V, Di Stefano C, Servo S, Zibetti M, Lopiano L, Maule S (2012) Neurogenic orthostatic hypotension as the initial feature of Parkinson disease. Clin Auton Res 22, 203–206. - PubMed
-
- Giannini G, Calandra-Buonaura G, Asioli GM, Cecere A, Barletta G, Mignani F, Ratti S, Guaraldi P, Provini F, Cortelli P (2018) The natural history of idiopathic autonomic failure: The IAF-BO cohort study. Neurology 91, e1245–e1254. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
