

Assessment of Physician Priorities in Delivery of Preventive Care
- PMID: 32716515
- PMCID: PMC8103855
- DOI: 10.1001/jamanetworkopen.2020.11677
Assessment of Physician Priorities in Delivery of Preventive Care
Abstract
Importance: Primary care physicians have limited time to discuss preventive care, but it is unknown how they prioritize recommended services.
Objective: To understand primary care physicians' prioritization of preventive services.
Design, setting, and participants: This online survey was administered to primary care physicians in a large health care system from March 17 to May 12, 2017. Physicians were asked whether they prioritize preventive services and which factors contribute to their choice (5-point Likert scale). Results were analyzed from July 8, 2017, to September 19, 2019.
Exposures: A 2 × 2 factorial design of 2 hypothetical patients: (1) a 50-year-old white woman with hypertension, type 2 diabetes, hyperlipidemia, obesity, a 30-pack-year history of smoking, and a family history of breast cancer; and (2) a 45-year-old black man with hypertension, hyperlipidemia, obesity, a 30-pack-year history of smoking, and a family history of colorectal cancer. Two visit lengths (40 minutes vs 20 minutes) were given. Each patient was eligible for at least 11 preventive services.
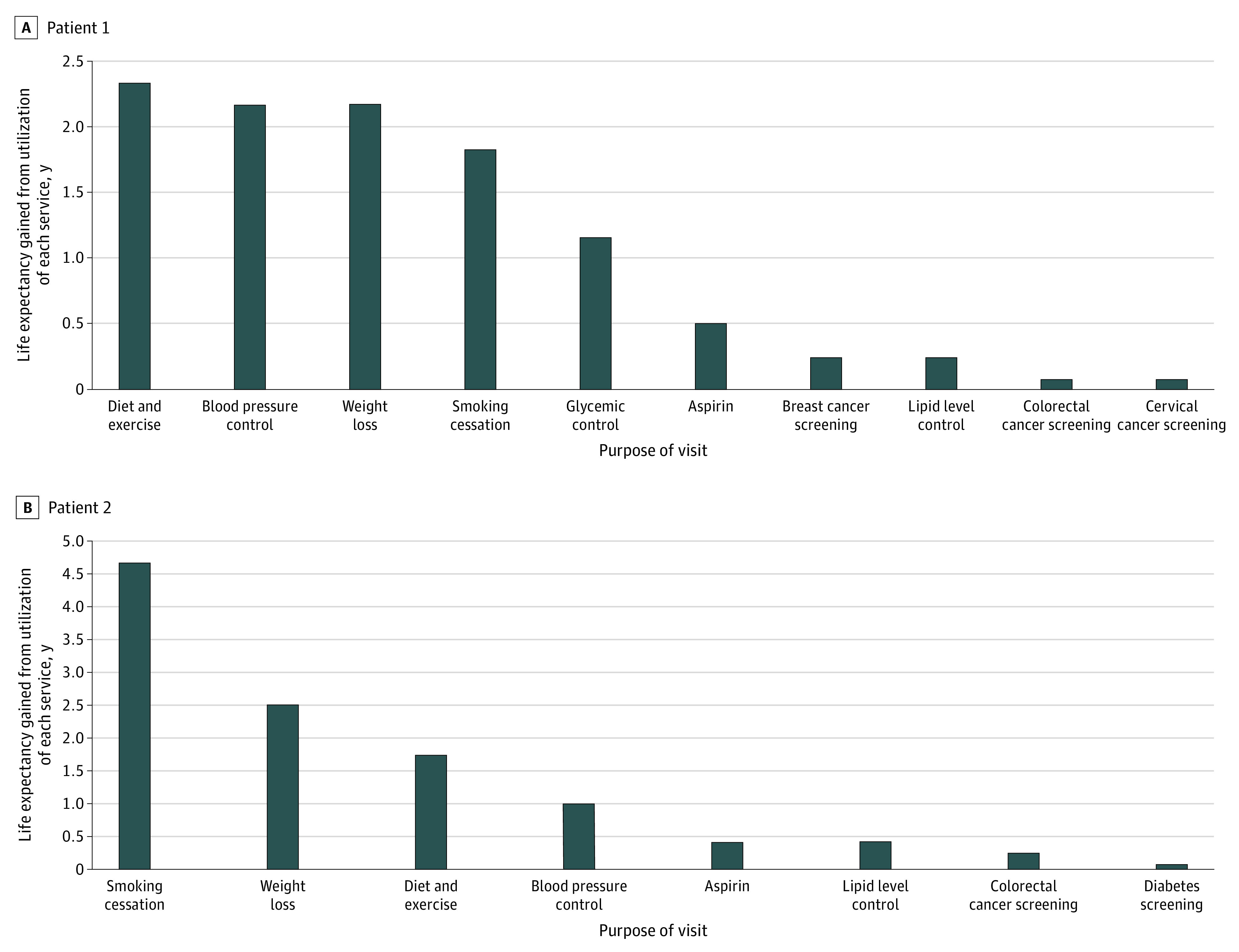
Main outcomes and measures: Physicians rated their likelihood of discussing each service during the visit and reported their top 3 priorities for patients 1 and 2. Physician choices were compared with the preventive services most likely to improve life expectancy, using a previously published mathematical model.
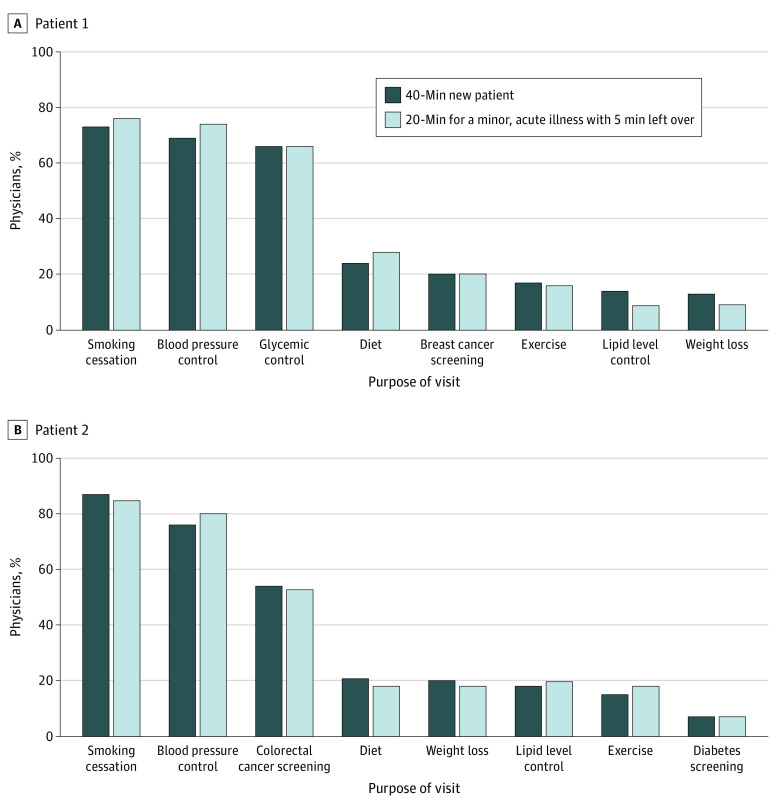
Results: Of 241 physicians, 137 responded (57%), of whom 74 (54%) were female and 85 (62%) were younger than 50 years. Physicians agreed they prioritized preventive services (mean score, 4.27 [95% CI, 4.12-4.42] of 5.00), mostly by ability to improve quality (4.56 [95% CI, 4.44-4.68] of 5.00) or length (4.53 [95% CI, 4.40-4.66] of 5.00) of life. Physicians reported more prioritization in the 20- vs 40-minute visit, indicating that they were likely to discuss fewer services during the shorter visit (median, 5 [interquartile range {IQR}, 3-8] vs 11 [IQR, 9-13] preventive services for patient 1, and 4 [IQR, 3-6] vs 9 [IQR, 8-11] for patient 2). Physicians reported similar top 3 priorities for both patients: smoking cessation, hypertension control, and glycemic control for patient 1 and smoking cessation, hypertension control, and colorectal cancer screening for patient 2. Physicians' top 3 priorities did not usually include diet and exercise or weight loss (ranked in their top 3 recommendations for either patient by only 48 physicians [35%]), although these were among the 3 preventive services most likely to improve life expectancy based on the mathematical model.
Conclusions and relevance: In this survey study, physicians prioritized preventive services under time constraints, but priorities did not vary across patients. Physicians did not prioritize lifestyle interventions despite large potential benefits. Future research should consider whether physicians and patients would benefit from guidance on preventive care priorities.
Conflict of interest statement
Figures
References
-
- US Preventive Services Task Force. USPSTF A and B Recommendations . February 2019. Accessed April 26, 2019. https://www.uspreventiveservicestaskforce.org/Page/Name/uspstf-a-and-b-r...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
