

Association of Cardiac Rehabilitation With All-Cause Mortality Among Patients With Cardiovascular Disease in the Netherlands
- PMID: 32716516
- PMCID: PMC12124693
- DOI: 10.1001/jamanetworkopen.2020.11686
Association of Cardiac Rehabilitation With All-Cause Mortality Among Patients With Cardiovascular Disease in the Netherlands
Abstract
Importance: Cardiac rehabilitation (CR) is an effective strategy to improve clinical outcomes, but it remains underused in some subgroups of patients with cardiovascular disease (CVD).
Objective: To investigate the implications of sex, age, socioeconomic status, CVD diagnosis, cardiothoracic surgery, and comorbidity for the association between CR participation and all-cause mortality.
Design, setting, and participants: Observational cohort study with patient enrollment between July 1, 2012, and December 31, 2017, and a follow-up to March 19, 2020. The dates of analysis were March to May 2020. This study was performed among Dutch patients with CVD with a multidisciplinary outpatient CR program indication and who were insured at Coöperatie Volksgezondheidszorg, one of the largest health insurance companies in the Netherlands. Among 4.1 million beneficiaries, patients with CVD with an acute coronary event (myocardial infarction or unstable angina pectoris), stable angina pectoris, chronic heart failure, or cardiothoracic surgery (coronary artery bypass grafting, valve replacement, or percutaneous coronary intervention) were identified by inpatient diagnosis codes and included in the study.
Main outcomes and measures: Cox proportional hazards models were used to evaluate the association between CR participation and all-cause mortality. Stabilized inverse propensity score weighting was used to account for patient and disease characteristics associated with CR participation.
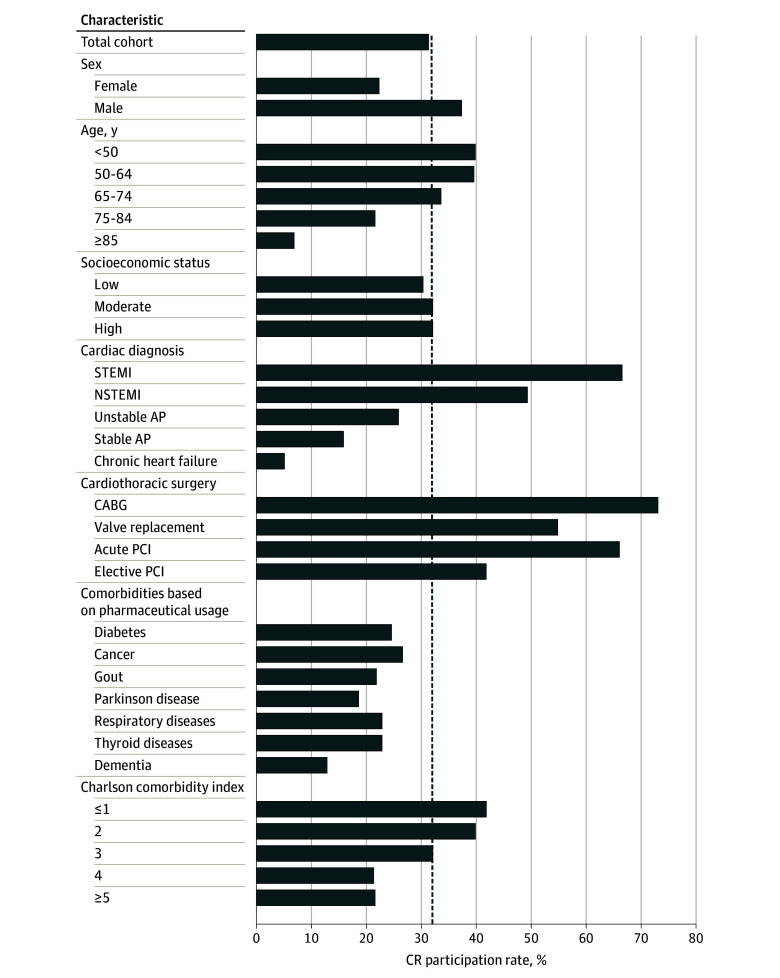
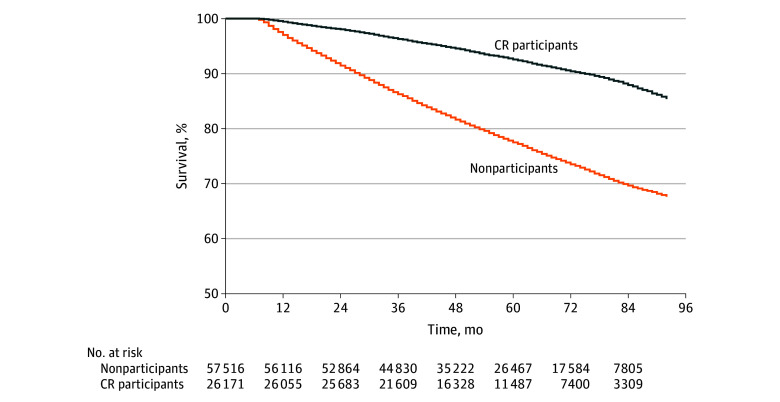
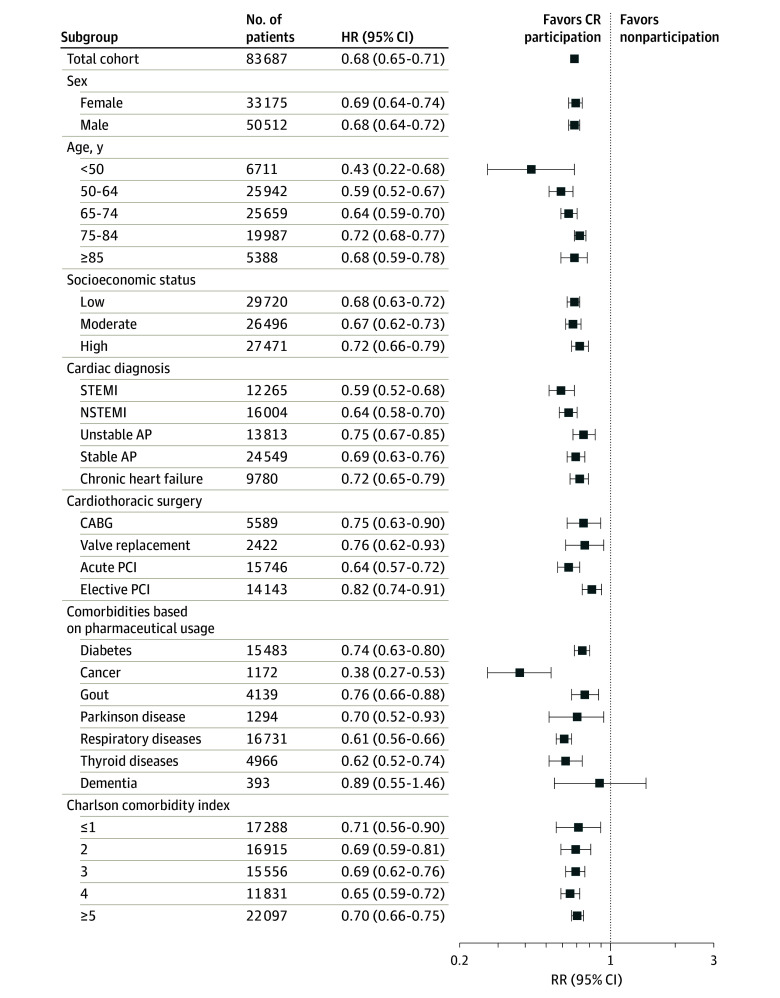
Results: Among 83 687 eligible patients with CVD (mean [SD] age, 67 [12] years; 60.4% [n = 50 512] men), only 31.3% (n = 26 171) participated in CR, with large variation across different subgroups (range, 5.1%-73.0%). During a mean (SD) of 4.7 (1.8) years of follow-up, 1966 CR participants (7.5%) and 13 443 CR nonparticipants (23.4%) died. After multivariable adjustment, CR participation was associated with a 32% lower risk of all-cause mortality (adjusted hazard ratio, 0.68; 95% CI, 0.65-0.71) compared with nonparticipation. Sex, age, socioeconomic status, and comorbidity did not alter risk reduction after CR participation, but a statistically significant interaction association was found across categories of CVD diagnosis and cardiothoracic surgery. Larger reductions in risk estimates for all-cause mortality were found after CR participation for STEMI (adjusted HR, 0.59; 95% CI, 0.52-0.68 vs 0.72; 95% CI, 0.65-0.79; P < .001), NSTEMI (adjusted HR, 0.64; 95% CI, 0.58-0.70 vs 0.72; 95% CI, 0.65-0.79; P < .001), and stable AP (adjusted HR, 0.69; 95% CI, 0.63-0.76 vs 0.72; 95% CI, 0.65-0.79; P < .001) compared with patients with chronic heart failure, whereas unstable AP had a smaller risk reduction (adjusted HR, 0.75; 95% CI, 0.67-0.85 vs 0.72; 95% CI, 0.65-0.79; P < .001).
Conclusions and relevance: In this cohort study, CR participation was associated with a 32% risk reduction in all-cause mortality, and this benefit was independent of sex, age, socioeconomic status, and comorbidity. These findings reinforce the importance of CR participation in secondary prevention and highlight the possibility that CR should be prescribed more widely to vulnerable patients with CVD, such as older adults with chronic diseases or multimorbidity.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
