

Population-Based Screening for Atrial Fibrillation
- PMID: 32716713
- PMCID: PMC7388078
- DOI: 10.1161/CIRCRESAHA.120.316341
Population-Based Screening for Atrial Fibrillation
Abstract
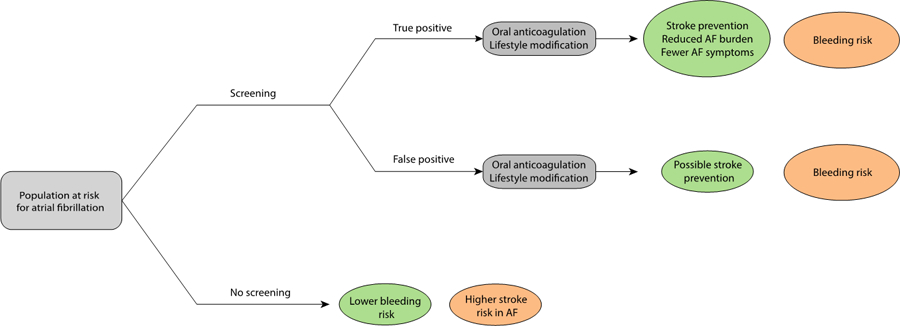
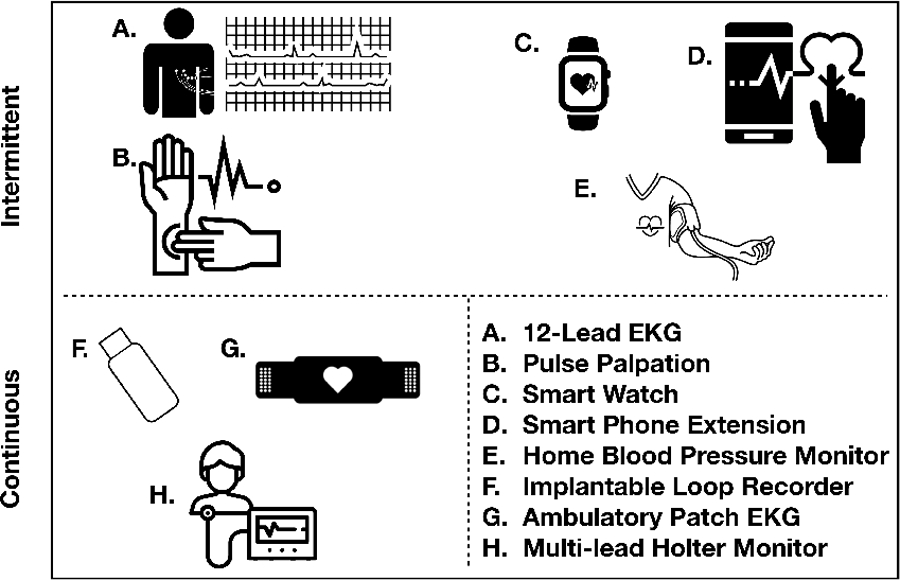
Atrial fibrillation (AF) is a common and morbid arrhythmia. Stroke is a major hazard of AF and may be preventable with oral anticoagulation. Yet since AF is often asymptomatic, many individuals with AF may be unaware and do not receive treatment that could prevent a stroke. Screening for AF has gained substantial attention in recent years as several studies have demonstrated that screening is feasible. Advances in technology have enabled a variety of approaches to facilitate screening for AF using both medical-prescribed devices as well as consumer electronic devices capable of detecting AF. Yet controversy about the utility of AF screening remains owing to concerns about potential harms resulting from screening in the absence of randomized data demonstrating effectiveness of screening on outcomes such as stroke and bleeding. In this review, we summarize current literature, present technology, population-based screening considerations, and consensus guidelines addressing the role of AF screening in practice.
Keywords: atrial fibrillation; atrial flutter; attention; stroke; technology.
Figures
References
-
- Chugh SS, Havmoeller R, Narayanan K, Singh D, Rienstra M, Benjamin EJ, Gillum RF, Kim Y-H, McAnulty JH, Zheng Z-J, Forouzanfar MH, Naghavi M, Mensah GA, Ezzati M, Murray CJL. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014;129:837–847. - PMC - PubMed
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Jordan LC, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, O’Flaherty M, Pandey A, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Spartano NL, Stokes A, Tirschwell DL, Tsao CW, Turakhia MP, VanWagner LB, Wilkins JT, Wong SS, Virani SS, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation. 2019;139:e56–e528. - PubMed
-
- Coyne KS, Paramore C, Grandy S, Mercader M, Reynolds M, Zimetbaum P. Assessing the direct costs of treating nonvalvular atrial fibrillation in the United States. Value Health. 2006;9:348–356. - PubMed
-
- Kim MH, Johnston SS, Chu B-C, Dalal MR, Schulman KL. Estimation of total incremental health care costs in patients with atrial fibrillation in the United States. Circ Cardiovasc Qual Outcomes. 2011;4:313–320. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
