

Multidisciplinary care for opioid dose reduction in patients with chronic non-cancer pain: A systematic realist review
- PMID: 32716982
- PMCID: PMC7384622
- DOI: 10.1371/journal.pone.0236419
Multidisciplinary care for opioid dose reduction in patients with chronic non-cancer pain: A systematic realist review
Abstract
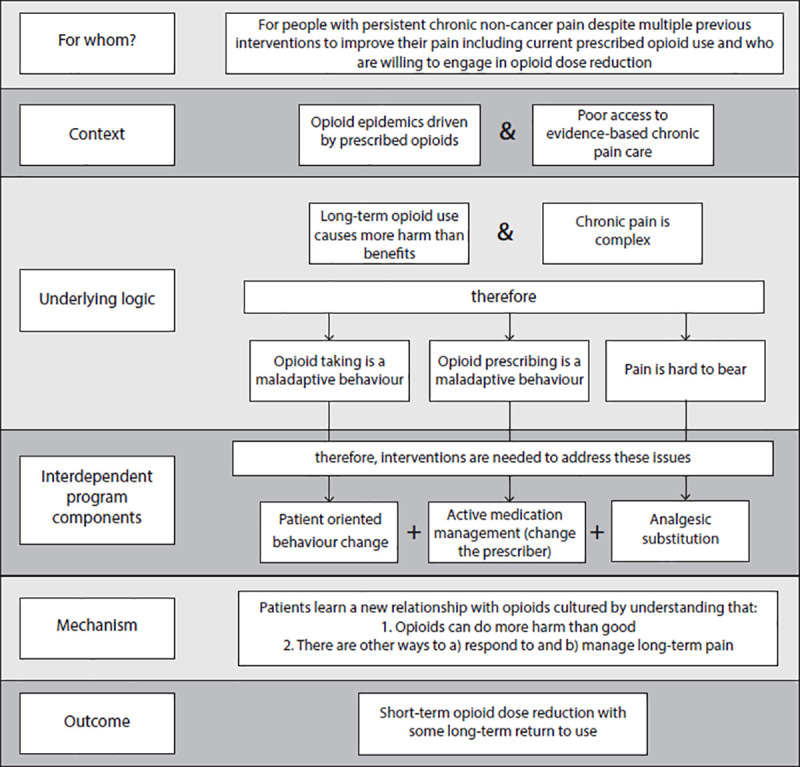
Context: Opioid related deaths are at epidemic levels in many developed nations globally. Concerns about the contribution of prescribed opioids, and particularly high-dose opioids, continue to mount as do initiatives to reduce prescribing. Evidence around opioid tapering, which can be challenging and potentially hazardous, is not well developed. A recent national guideline has recognized this and recommended referral to multidisciplinary care for challenging cases of opioid tapering. However, multidisciplinary care for opioid tapering is not well understood or defined.
Objective: Identify the existing literature on any multidisciplinary care programs that evaluate impact on opioid use, synthesize how these programs work and clarify whom they benefit.
Study design: Systematic rapid realist review.
Dataset: Bibliographic databases (MEDLINE, EMBASE, CINAHL, PsycINFO, Cochrane Library), grey literature, reference hand search and formal expert consultation.
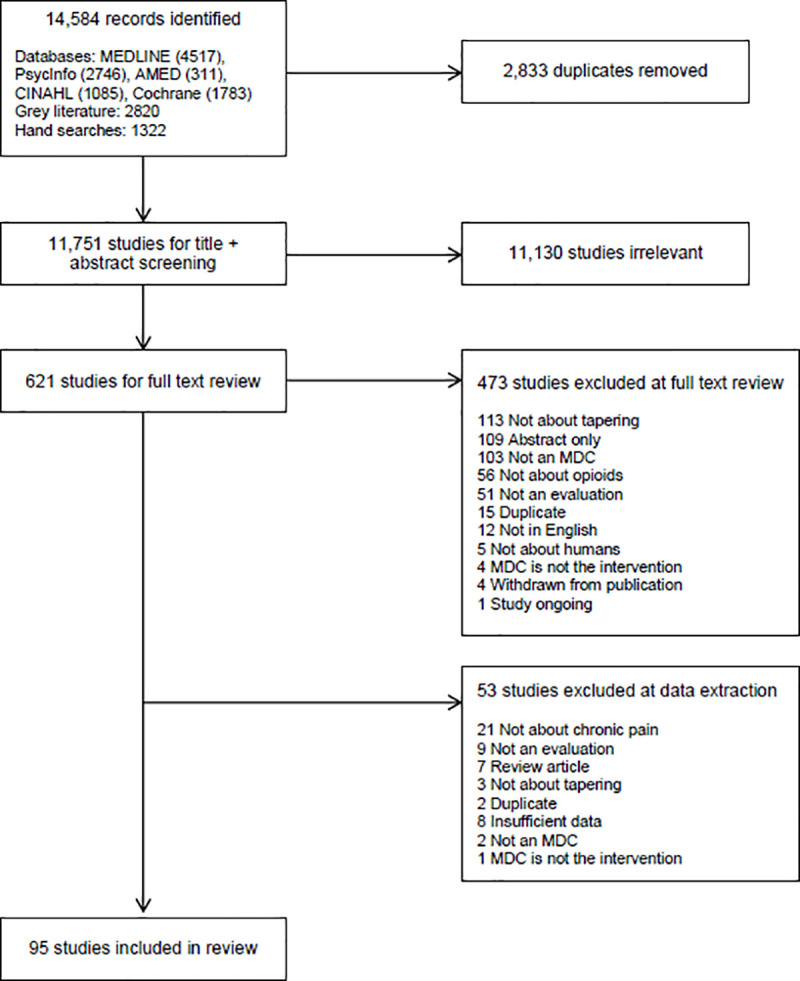
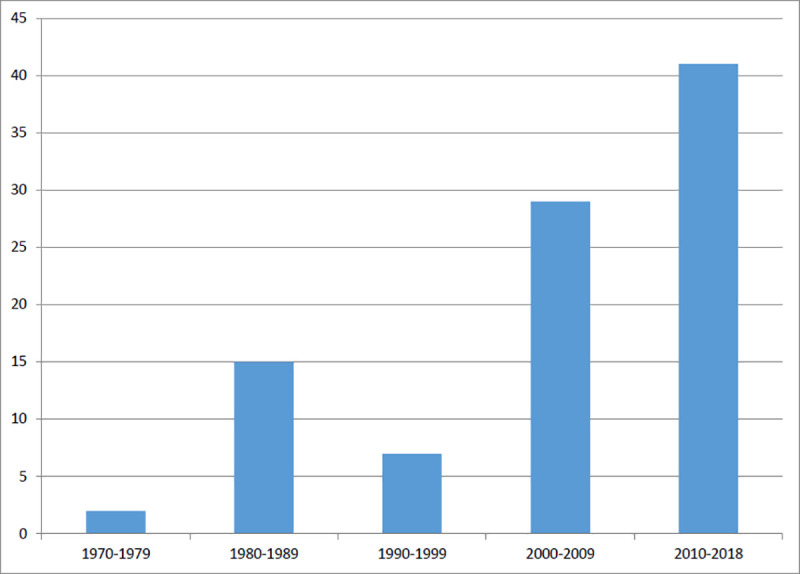
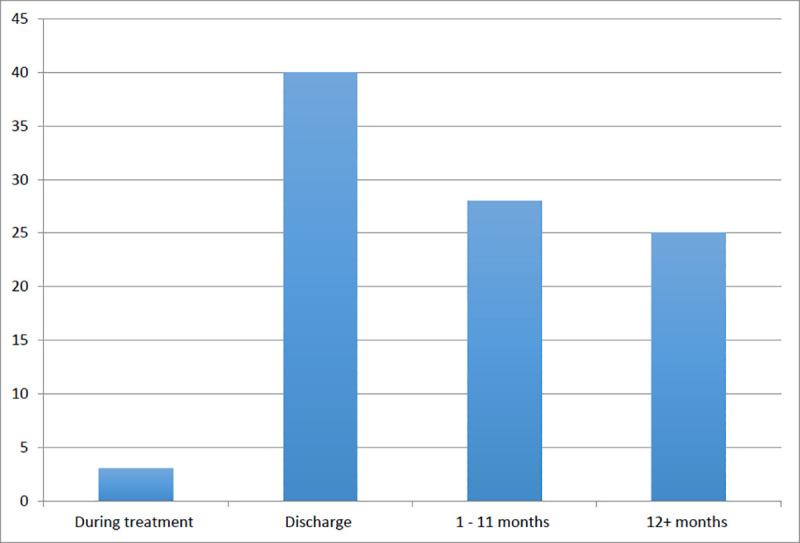
Results: 95 studies were identified. 75% of the programs were from the United States and the majority (n = 62) were published after 2000. A minority (n = 23) of programs reported on >12 month opioid use outcomes. There were three necessary but insufficient mechanisms common to all programs: pain relief, behavior change and active medication management. Programs that did not include a combination of all three mechanisms did not result in opioid dose reductions. A concerning 20-40% of subjects resumed opioid use within one year of program completion.
Conclusions: Providing alternative analgesia is insufficient for reducing opioid doses. Even high quality primary care multidisciplinary care programs do not reduce prescribed opioid use unless there is active medication management accomplished by changing the primary opioid prescriber. Rates of return to use of opioids from these programs are very concerning in the current context of a highly potent and lethal street drug supply. This contextual factor may be powerful enough to undermine the modest benefits of opioid dose reduction via multidisciplinary care.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Centers for Disease Control and Prevention. Drug overdose deaths: Centers for Disease Control and Prevention 2019 [cited 2019].
-
- Leifman H. Drug-related deaths in Sweden: Estimations of trends, effects of changes in recording practices and studies of drug patterns. Stockholm: Centralförbundet för alcohol-och narkotikaupplysning, 2016. Contract No.: Rapport 158.
-
- Ontario Agency of Health Protection and Promotion (Public Health Ontario), Office of the Chief Coroner, Ontario Forensic Pathology Service, Ontario Drug Policy Research Network. Opioid mortality surveillance report: Analysis of opioid-related deaths in Ontario July 2017—June 2018 Toronto, ON: 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
