

Coronary physiology before and after chronic total occlusion treatment: what does it tell us?
- PMID: 32720123
- PMCID: PMC7782651
- DOI: 10.1007/s12471-020-01470-6
Coronary physiology before and after chronic total occlusion treatment: what does it tell us?
Abstract
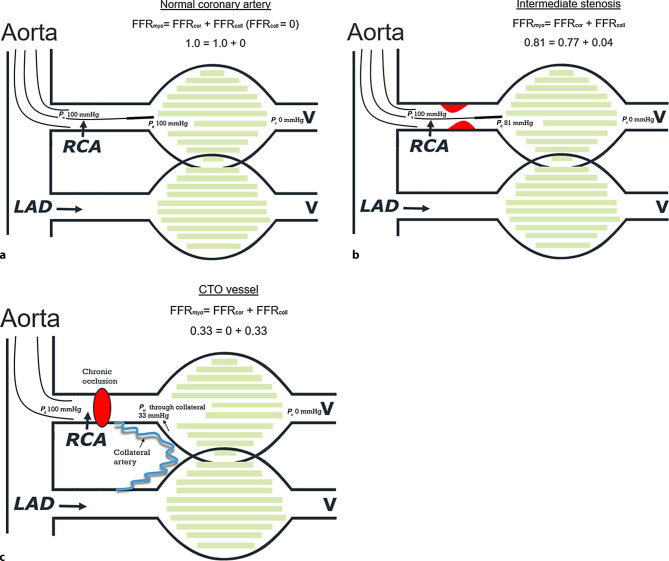
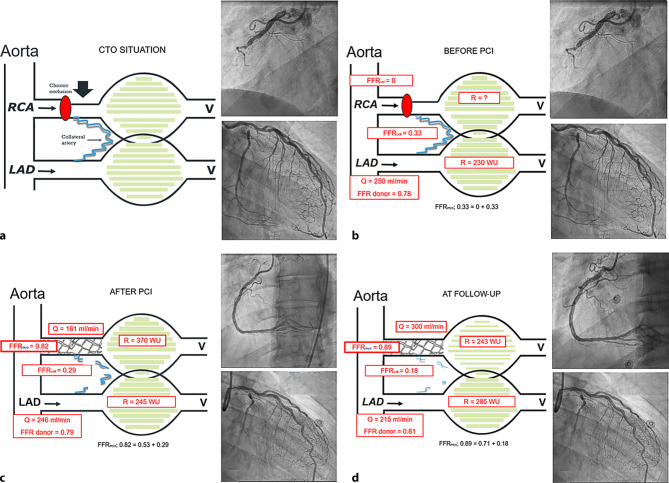
Studies performed in the last two decades demonstrate that after successful percutaneous coronary intervention (PCI) of a chronically occluded coronary artery, the physiology of the chronic total occlusion (CTO) vessel and dependent microvasculature does not normalise immediately but improves significantly over time. Generally, there is an increase in fractional flow reserve (FFR) in the CTO artery, a decrease in collateral blood supply and an increase in FFR in the donor artery accompanied by an increase in blood flow and decrease in microvascular resistance in the myocardium supplied by the CTO vessel. Analogous to these physiological changes, positive remodelling of the distal CTO artery also occurs over time, and intravascular imaging can be helpful for analysing distal vessel parameters. Follow-up coronary angiography with physiological measurements after several weeks to months can be helpful and informative in a subset of patients in order to decide upon the necessity for treatment of residual coronary artery stenosis in the vessel distal to the CTO or in the contralateral donor artery, as well as in deciding whether stent optimisation is indicated. We suggest that such physiological guidance of CTO procedures avoids unnecessary overtreatment during the initial procedure, guides interventions at follow-up, and improves our understanding of what PCI in CTO means.
Keywords: Chronic total occlusion; Coronary flow reserve; Fractional flow reserve; Percutaneous coronary intervention; Physiology.
Conflict of interest statement
N.H.J. Pijls has received institutional research grants from Abbott and Hexacath, is a consultant for Abbott, Opsens and GE, and minor shareholder in Philips, ASML, Heartflow. D.C.J. Keulards, P.J. Vlaar, I. Wijnbergen and K. Teeuwen declare that they have no competing interests.
Figures

References
-
- Stuijfzand WJ, Driessen RS, Raijmakers PG, Rijnierse MT, Maeremans J, Hollander MR, et al. Prevalence of ischaemia in patients with a chronic total occlusion and preserved left ventricular ejection fraction. Eur Heart J Cardiovasc Imaging. 2017;18:1025–1033. doi: 10.1093/ehjci/jew188. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
