

Advances in Therapeutic Approaches for Spontaneous Intracerebral Hemorrhage
- PMID: 32720246
- PMCID: PMC7851203
- DOI: 10.1007/s13311-020-00902-w
Advances in Therapeutic Approaches for Spontaneous Intracerebral Hemorrhage
Abstract
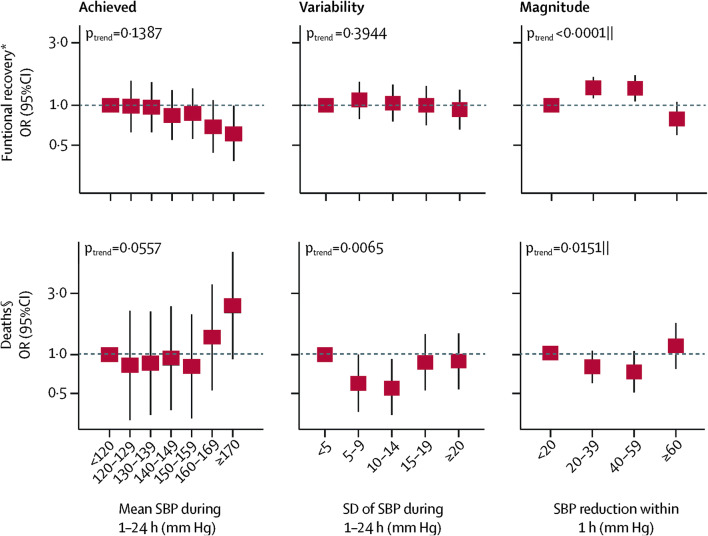
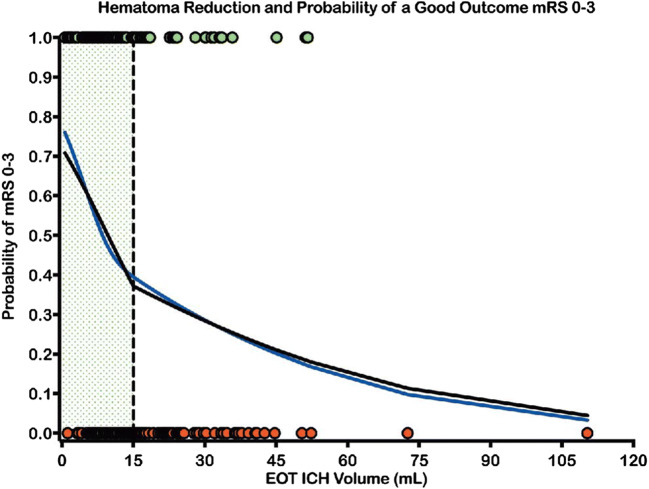
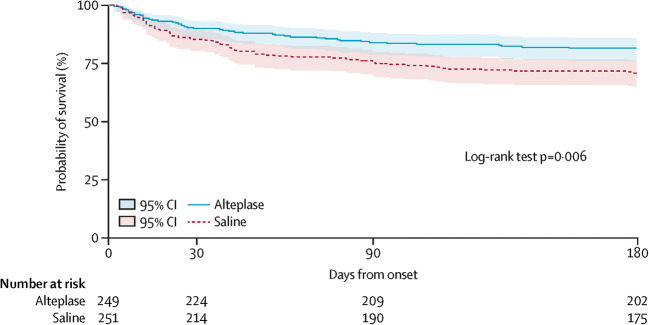
Spontaneous intracerebral hemorrhage (ICH) results in high rates of morbidity and mortality, with intraventricular hemorrhage (IVH) being associated with even worse outcomes. Therapeutic interventions in acute ICH have continued to emerge with focus on arresting hemorrhage expansion, clot volume reduction of both intraventricular and parenchymal hematomas, and targeting perihematomal edema and inflammation. Large randomized controlled trials addressing the effectiveness of rapid blood pressure lowering, hemostatic therapy with platelet transfusion, and other clotting complexes and hematoma volume reduction using minimally invasive techniques have impacted clinical guidelines. We review the recent evolution in the management of acute spontaneous ICH, discussing which interventions have been shown to be safe and which may potentially improve outcomes.
Keywords: Fibrinolysis; Intracerebral hemorrhage; Intraventricular hemorrhage; Outcomes; Stroke.
Figures
References
-
- Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8:355–369. - PubMed
-
- Kazui S, Minematsu K, Yamamoto H, Sawada T, Yamaguchi T. Predisposing factors to enlargement of spontaneous intracerebral hematoma. Stroke. 1997;28:2370–2375. - PubMed
-
- Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013;368:2355–2365. - PubMed
-
- Hemphill JC, 3rd, Greenberg SM, Anderson CS, et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2015;46:2032–2060. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
