

The global burden of disease attributable to high body mass index in 195 countries and territories, 1990-2017: An analysis of the Global Burden of Disease Study
- PMID: 32722671
- PMCID: PMC7386577
- DOI: 10.1371/journal.pmed.1003198
The global burden of disease attributable to high body mass index in 195 countries and territories, 1990-2017: An analysis of the Global Burden of Disease Study
Abstract
Background: Obesity represents an urgent problem that needs to be properly addressed, especially among children. Public and global health policy- and decision-makers need timely, reliable quantitative information to develop effective interventions aimed at counteracting the burden generated by high body mass index (BMI). Few studies have assessed the high-BMI-related burden on a global scale.
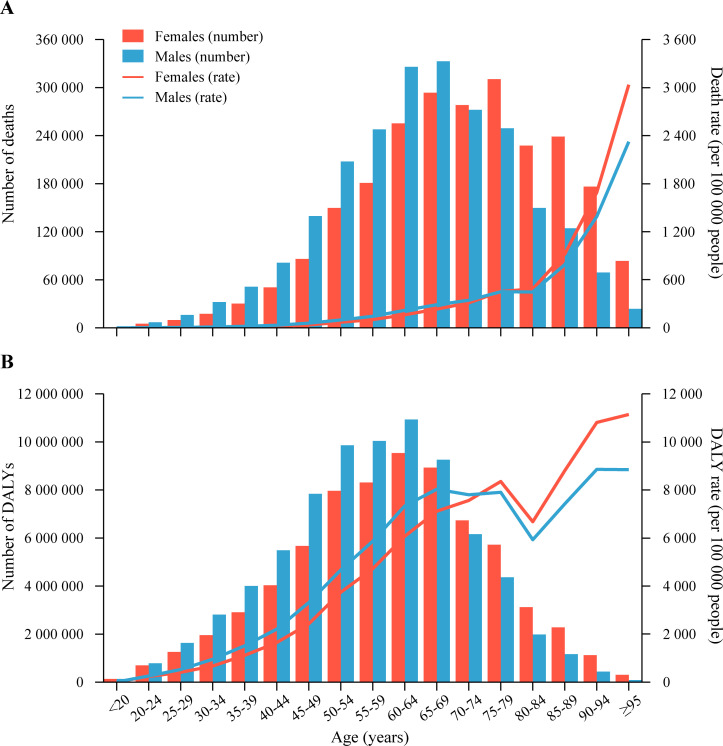
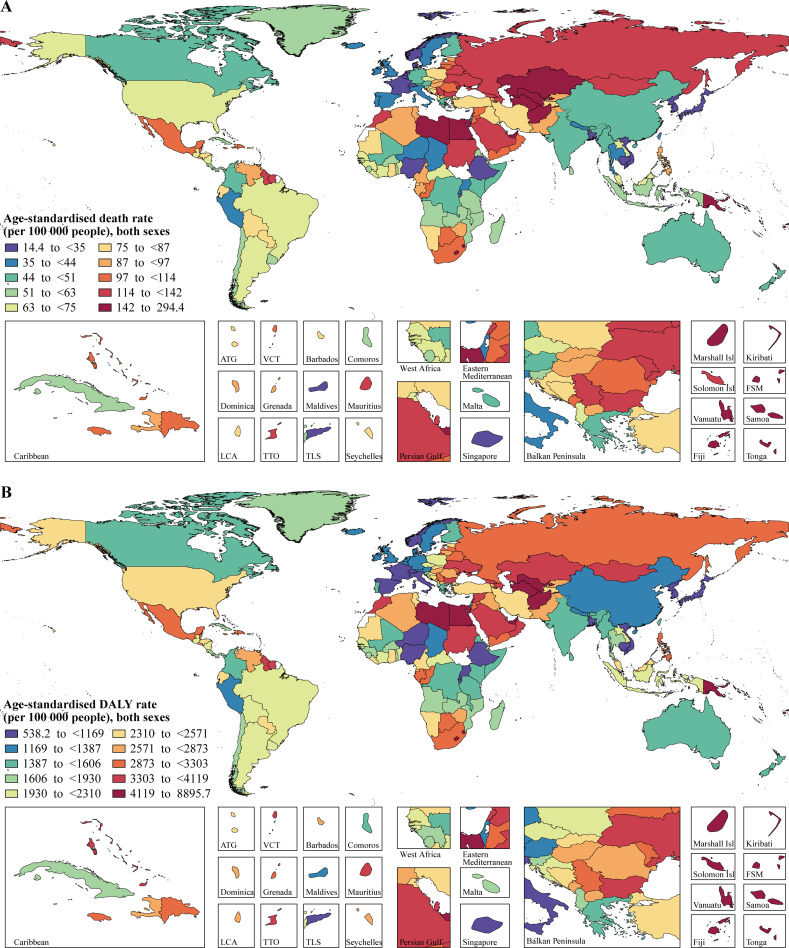
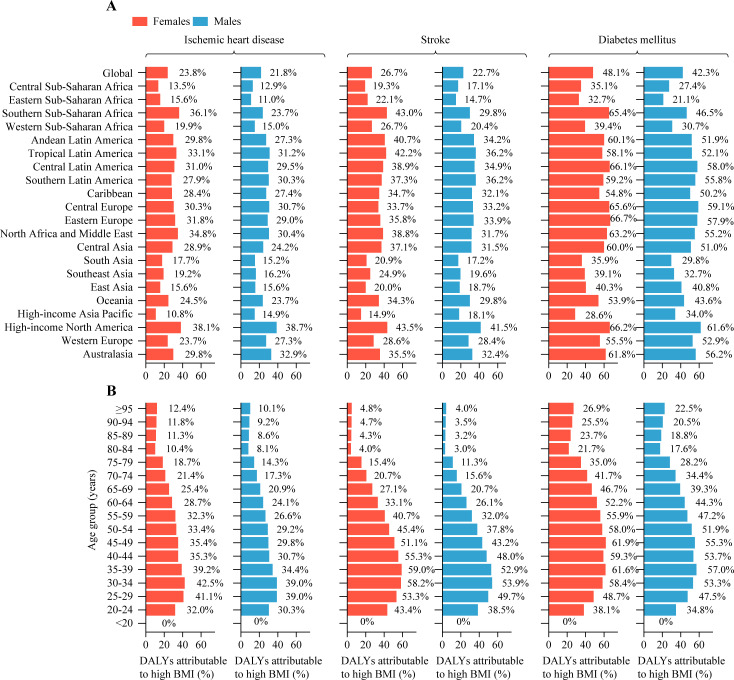
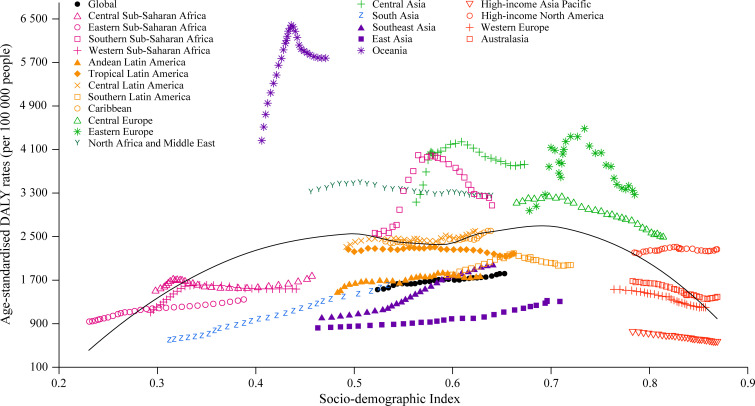
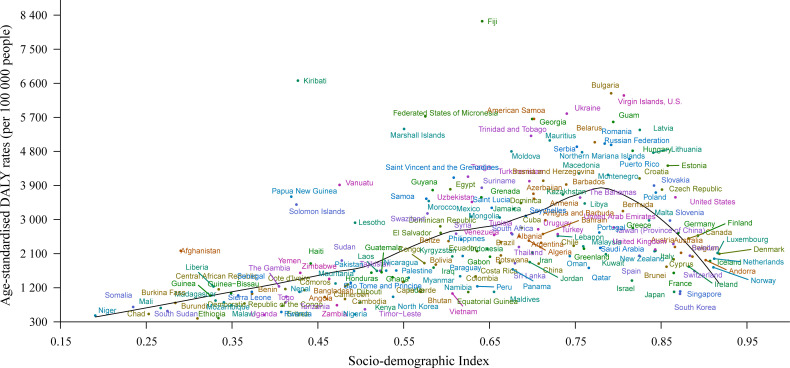
Methods and findings: Following the methodology framework and analytical strategies used in the Global Burden of Disease Study (GBD) 2017, the global deaths and disability-adjusted life years (DALYs) attributable to high BMI were analyzed by age, sex, year, and geographical location and by Socio-demographic Index (SDI). All causes of death and DALYs estimated in GBD 2017 were organized into 4 hierarchical levels: level 1 contained 3 broad cause groupings, level 2 included more specific categories within the level 1 groupings, level 3 comprised more detailed causes within the level 2 categories, and level 4 included sub-causes of some level 3 causes. From 1990 to 2017, the global deaths and DALYs attributable to high BMI have more than doubled for both females and males. However, during the study period, the age-standardized rate of high-BMI-related deaths remained stable for females and only increased by 14.5% for males, and the age-standardized rate of high-BMI-related DALYs only increased by 12.7% for females and 26.8% for males. In 2017, the 6 leading GBD level 3 causes of high-BMI-related DALYs were ischemic heart disease, stroke, diabetes mellitus, chronic kidney disease, hypertensive heart disease, and low back pain. For most GBD level 3 causes of high-BMI-related DALYs, high-income North America had the highest attributable proportions of age-standardized DALYs due to high BMI among the 21 GBD regions in both sexes, whereas the lowest attributable proportions were observed in high-income Asia Pacific for females and in eastern sub-Saharan Africa for males. The association between SDI and high-BMI-related DALYs suggested that the lowest age-standardized DALY rates were found in countries in the low-SDI quintile and high-SDI quintile in 2017, and from 1990 to 2017, the age-standardized DALY rates tended to increase in regions with the lowest SDI, but declined in regions with the highest SDI, with the exception of high-income North America. The study's main limitations included the use of information collected from some self-reported data, the employment of cutoff values that may not be adequate for all populations and groups at risk, and the use of a metric that cannot distinguish between lean and fat mass.
Conclusions: In this study, we observed that the number of global deaths and DALYs attributable to high BMI has substantially increased between 1990 and 2017. Successful population-wide initiatives targeting high BMI may mitigate the burden of a wide range of diseases. Given the large variations in high-BMI-related burden of disease by SDI, future strategies to prevent and reduce the burden should be developed and implemented based on country-specific development status.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Ding D, Rogers K, van der Ploeg H, Stamatakis E, Bauman AE. Traditional and Emerging Lifestyle Risk Behaviors and All-Cause Mortality in Middle-Aged and Older Adults: Evidence from a Large Population-Based Australian Cohort. PLoS Med. 2015;12(12):e1001917 10.1371/journal.pmed.1001917 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
