

Association of bariatric surgery with all-cause mortality and incidence of obesity-related disease at a population level: A systematic review and meta-analysis
- PMID: 32722673
- PMCID: PMC7386646
- DOI: 10.1371/journal.pmed.1003206
Association of bariatric surgery with all-cause mortality and incidence of obesity-related disease at a population level: A systematic review and meta-analysis
Abstract
Background: Previous clinical trials and institutional studies have demonstrated that surgery for the treatment of obesity (termed bariatric or metabolic surgery) reduces all-cause mortality and the development of obesity-related diseases such as type 2 diabetes mellitus (T2DM), hypertension, and dyslipidaemia. The current study analysed large-scale population studies to assess the association of bariatric surgery with long-term mortality and incidence of new-onset obesity-related disease at a national level.
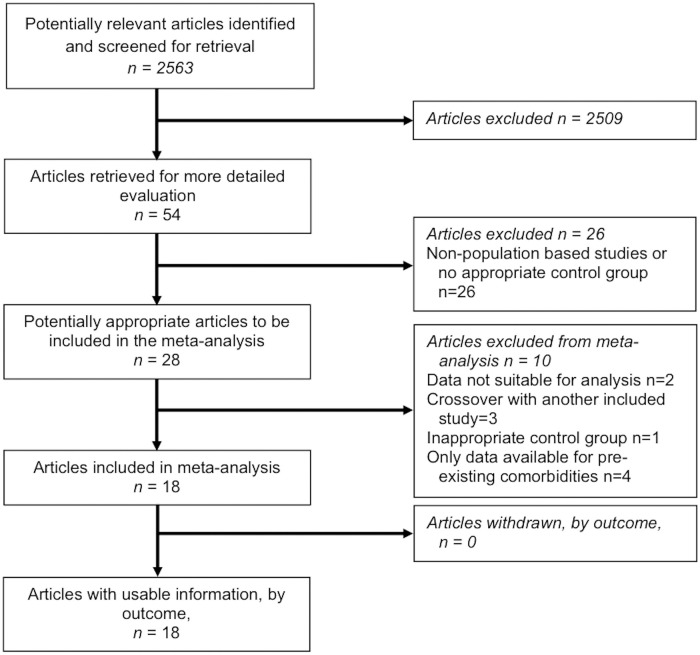
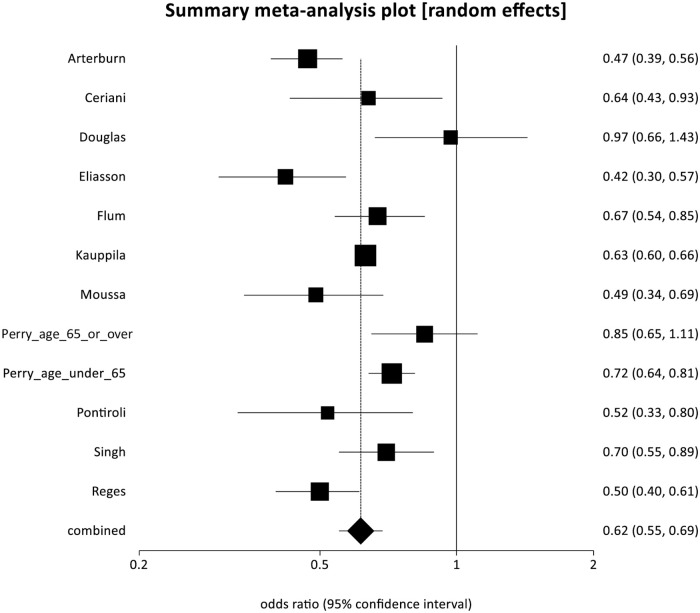
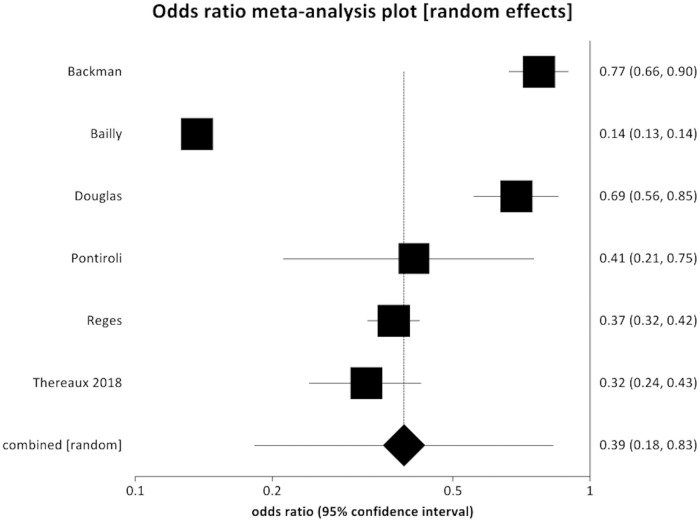
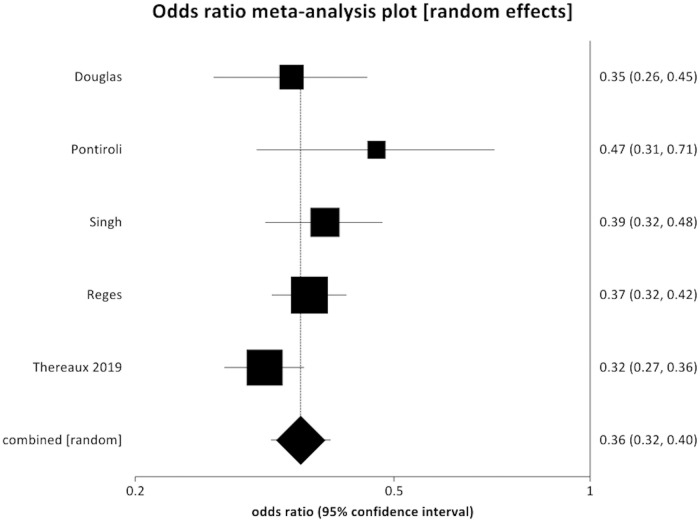
Methods and findings: A systematic literature search of Medline (via PubMed), Embase, and Web of Science was performed. Articles were included if they were national or regional administrative database cohort studies reporting comparative risk of long-term mortality or incident obesity-related diseases for patients who have undergone any form of bariatric surgery compared with an appropriate control group with a minimum follow-up period of 18 months. Meta-analysis of hazard ratios (HRs) was performed for mortality risk, and pooled odds ratios (PORs) were calculated for discrete variables relating to incident disease. Eighteen studies were identified as suitable for inclusion. There were 1,539,904 patients included in the analysis, with 269,818 receiving bariatric surgery and 1,270,086 control patients. Bariatric surgery was associated with a reduced rate of all-cause mortality (POR 0.62, 95% CI 0.55 to 0.69, p < 0.001) and cardiovascular mortality (POR 0.50, 95% CI 0.35 to 0.71, p < 0.001). Bariatric surgery was strongly associated with reduced incidence of T2DM (POR 0.39, 95% CI 0.18 to 0.83, p = 0.010), hypertension (POR 0.36, 95% CI 0.32 to 0.40, p < 0.001), dyslipidaemia (POR 0.33, 95% CI 0.14 to 0.80, p = 0.010), and ischemic heart disease (POR 0.46, 95% CI 0.29 to 0.73, p = 0.001). Limitations of the study include that it was not possible to account for unmeasured variables, which may not have been equally distributed between patient groups given the non-randomised design of the studies included. There was also heterogeneity between studies in the nature of the control group utilised, and potential adverse outcomes related to bariatric surgery were not specifically examined due to a lack of available data.
Conclusions: This pooled analysis suggests that bariatric surgery is associated with reduced long-term all-cause mortality and incidence of obesity-related disease in patients with obesity for the whole operated population. The results suggest that broader access to bariatric surgery for people with obesity may reduce the long-term sequelae of this disease and provide population-level benefits.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Various effects of bariatric surgery on mortality and incidences of obesity-related co-morbidities at different follow-up times at a population level.Surg Obes Relat Dis. 2021 Jul;17(7):1393. doi: 10.1016/j.soard.2021.04.006. Epub 2021 Apr 9. Surg Obes Relat Dis. 2021. PMID: 33962873 No abstract available.
References
-
- World Health Organization. Global Health Observatory (GHO) data: overweight and obesity. Geneva: World Health Organization; 2020. [cited 2020 Apr 30]. http://www.who.int/gho/ncd/risk_factors/overweight/en/.
-
- NHS Digital. Statistics on obesity, physical activity and diet. Leeds: NHS Digital; 2017. [cited 2020 Apr 30]. https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
