

Burden of hepatitis E virus infection in pregnancy and maternofoetal outcomes: a systematic review and meta-analysis
- PMID: 32723309
- PMCID: PMC7388479
- DOI: 10.1186/s12884-020-03116-2
Burden of hepatitis E virus infection in pregnancy and maternofoetal outcomes: a systematic review and meta-analysis
Abstract
Background: There is still a dearth of knowledge on the burden of HEV infection in the global population of pregnant women. Therefore, we conducted a systematic review and meta-analysis to estimate the global burden of HEV infection in pregnancy.
Methods: We searched PubMed, Embase, Web of Knowledge, and Global Index Medicus to identify articles published until January 26, 2020. We considered cross-sectional, case-control, and cohort studies reporting the immunoglobulins M HEV seroprevalence in asymptomatic and symptomatic (jaundice or elevated transaminases) pregnant women or investigating the association between HEV infection and maternofoetal outcomes. We used a random-effects model to pool studies. This review was registered with PROSPERO, CRD42018093820.
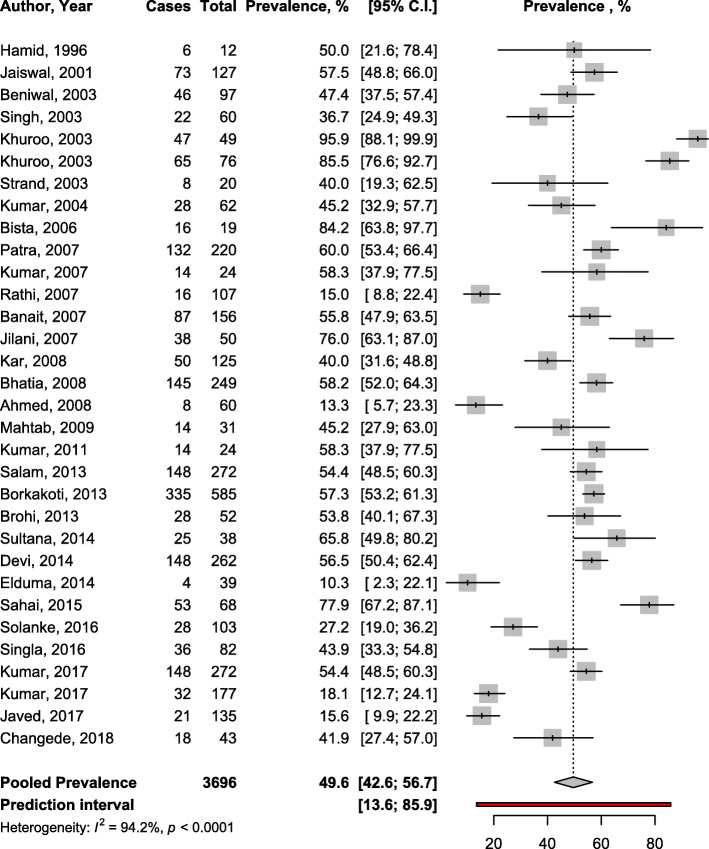
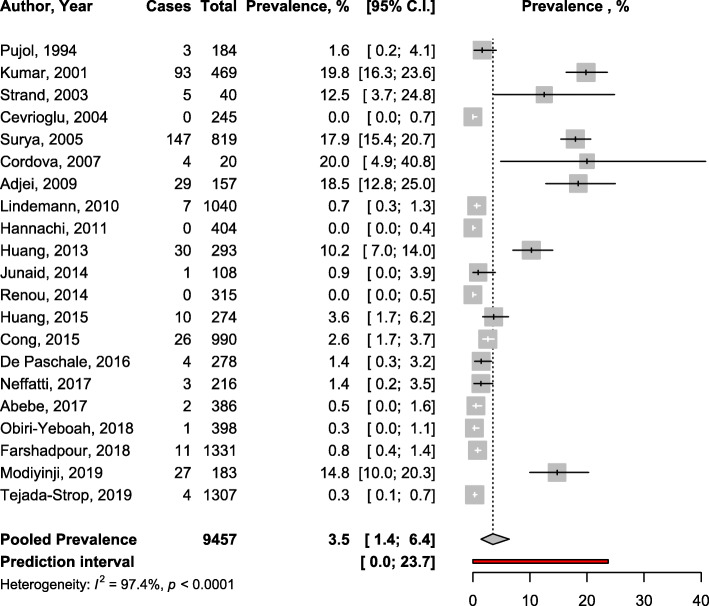
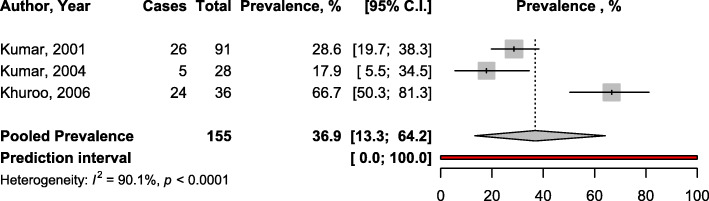
Results: For HEV prevalence estimates, we included 52 studies (11,663 pregnant women). The seroprevalence was 3.5% (95% confidence interval: 1.4-6.4) in asymptomatic women (most of whom from high endemic areas). The prevalence in symptomatic women was 49.6% (42.6-56.7) with data only from HEV high endemic countries. In the multivariable meta-regression model, the prevalence was higher in symptomatic women compared to asymptomatic (adjusted prevalence odds ratio [aPOR]: 1.76; 95%CI: 1.61-1.91) and decreased with increasing year of publication (by 10-year) (aPOR: 0.90; 95%CI: 0.84-0.96). The proportion of HEV vertical transmission was 36.9% (13.3-64.2). Risk of bias was low, moderate and high respectively in 12 (23%), 37 (70%), and 4 studies (7%) addressing HEV prevalence estimation. HEV infection was associated with maternal deaths (pooled OR 7.17; 3.32-15.47), low birth weight (OR: 3.23; 1.71-6.10), small for gestational age (OR: 3.63; 1.25-10.49), preterm < 32 weeks (OR: 4.18; 1.23-14.20), and preterm < 37 weeks (OR: 3.45; 2.32-5.13), stillbirth (OR: 2.61; 1.64-4.14), intrauterine deaths (OR: 3.07; 2.13-4.43), and not with miscarriage (OR: 1.74; 0.77-3.90). All studies which assessed the association between HEV infection and maternofoetal outcomes had a moderate risk of bias.
Conclusions: Findings from this study are suggestive of a high burden of HEV infection in pregnancy in high endemic countries, its association with poor maternofoetal outcomes, and a high rate of vertical transmission. This study supports the need for specific strategies to prevent exposure of pregnant women to HEV infection, especially in high endemic areas.
Keywords: Hepatitis E; Intrauterine deaths; Low birth weight; Maternal deaths; Miscarriage; Pregnancy; Preterm; Small for gestational age; Vertical transmission; Women health.
Conflict of interest statement
None.
Figures


References
-
- World Health Organization. Global Health sector strategy on viral hepatitis 2016-2021: Towards ending viral hepatitis. WHO: 2016. https://apps.who.int/iris/bitstream/handle/10665/246177/WHO-HIV-2016.06-....
-
- WHO: Global Hepatitis Report: Prevent, test and treat. http://apps.who.int/iris/bitstream/handle/10665/255016/9789241565455-eng.... Accessed on Jul 6, 2018.
-
- WHO: Hepatitis E: Key facts. http://www.who.int/news-room/fact-sheets/detail/hepatitis-e. Accessed on June 9, 2018.
-
- Dalton HR, Izopet J. Transmission and epidemiology of hepatitis E virus genotype 3 and 4 infections. Cold Spring Harbor Perspect Med. 2018;18(11):a032144. https://pubmed.ncbi.nlm.nih.gov/29530946/. - PMC - PubMed
-
- Izopet J, Lhomme S, Chapuy-Regaud S, Mansuy JM, Kamar N, Abravanel F. HEV and transfusion-recipient risk. VHE Risque receveur. 2017;24(3):176–181. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
