

Airway pressure morphology and respiratory muscle activity during end-inspiratory occlusions in pressure support ventilation
- PMID: 32723356
- PMCID: PMC7385937
- DOI: 10.1186/s13054-020-03169-x
Airway pressure morphology and respiratory muscle activity during end-inspiratory occlusions in pressure support ventilation
Abstract
Background: The driving pressure of the respiratory system is a valuable indicator of global lung stress during passive mechanical ventilation. Monitoring lung stress in assisted ventilation is indispensable, but achieving passive conditions in spontaneously breathing patients to measure driving pressure is challenging. The accuracy of the morphology of airway pressure (Paw) during end-inspiratory occlusion to assure passive conditions during pressure support ventilation has not been examined.
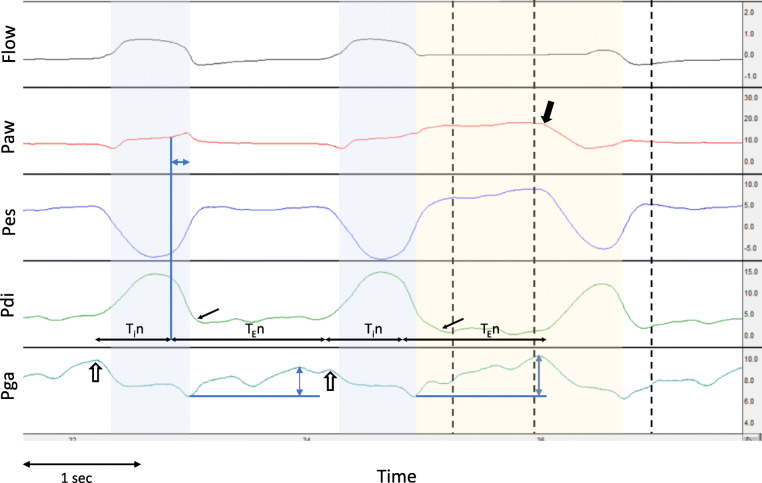
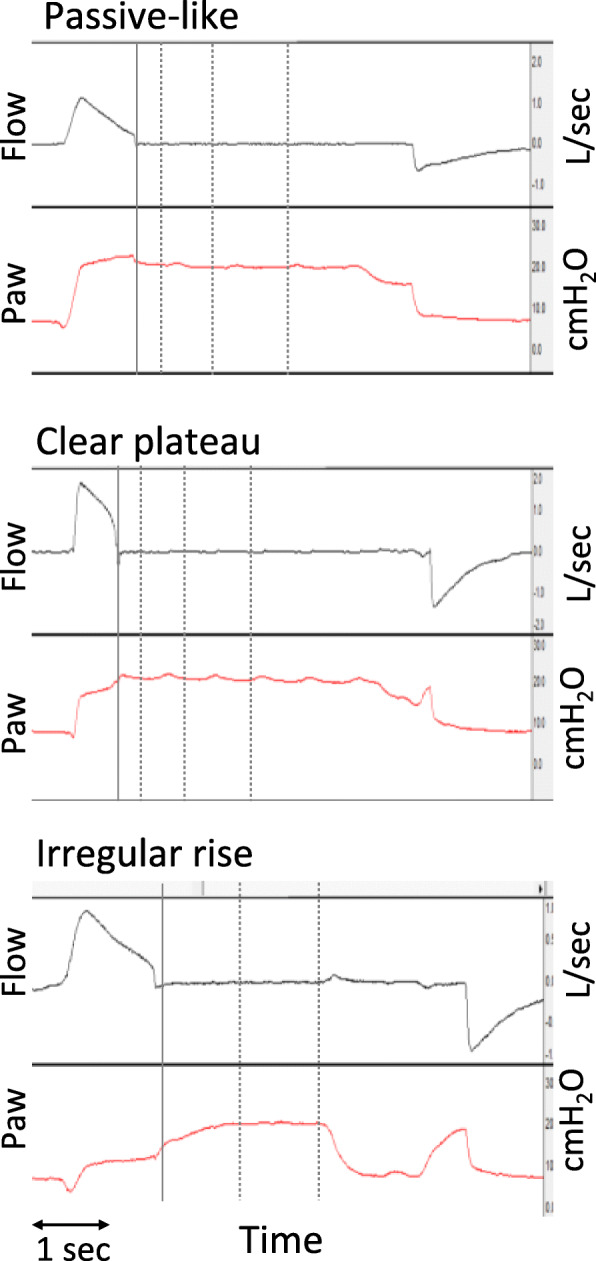
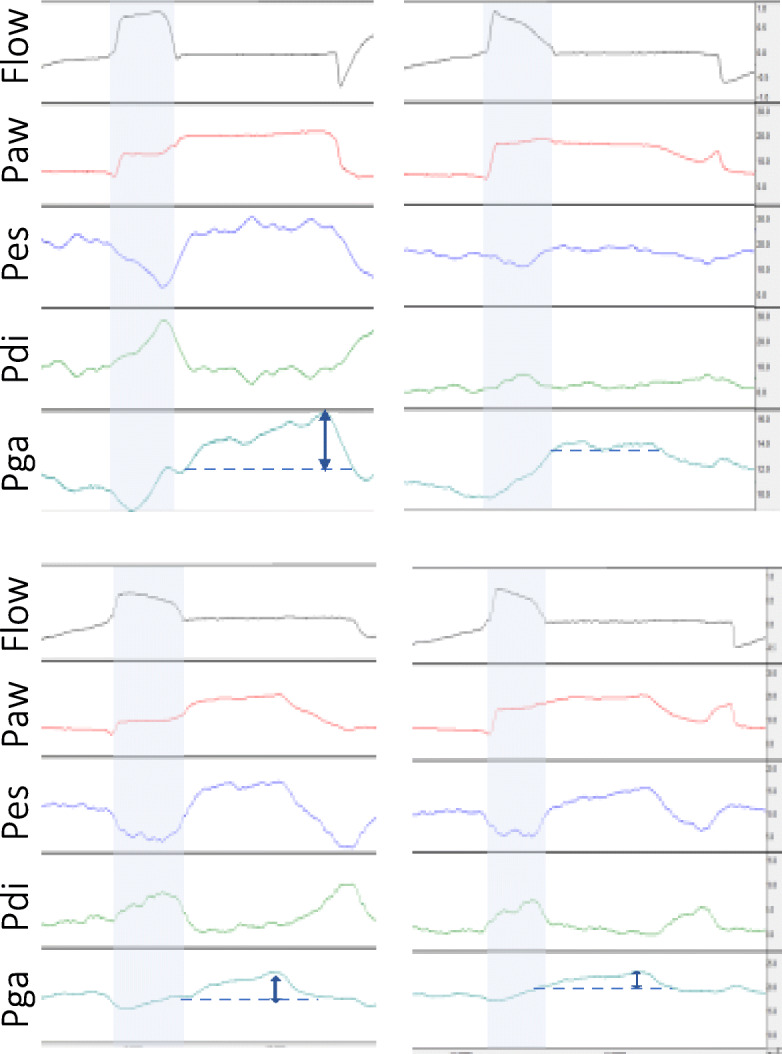
Methods: Retrospective analysis of end-inspiratory occlusions obtained from critically ill patients during pressure support ventilation. Flow, airway, esophageal, gastric, and transdiaphragmatic pressures were analyzed. The rise of gastric pressure during occlusion with a constant/decreasing transdiaphragmatic pressure was used to identify and quantify the expiratory muscle activity. The Paw during occlusion was classified in three patterns, based on the differences at three pre-defined points after occlusion (0.3, 1, and 2 s): a "passive-like" decrease followed by plateau, a pattern with "clear plateau," and an "irregular rise" pattern, which included all cases of late or continuous increase, with or without plateau.
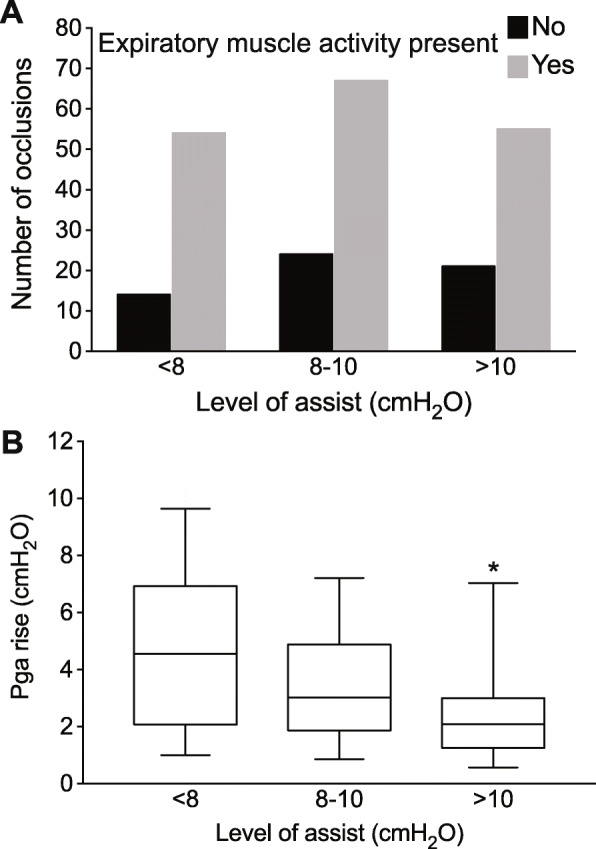
Results: Data from 40 patients and 227 occlusions were analyzed. Expiratory muscle activity during occlusion was identified in 79% of occlusions, and at all levels of assist. After classifying occlusions according to Paw pattern, expiratory muscle activity was identified in 52%, 67%, and 100% of cases of Paw of passive-like, clear plateau, or irregular rise pattern, respectively. The driving pressure was evaluated in the 133 occlusions having a passive-like or clear plateau pattern in Paw. An increase in gastric pressure was present in 46%, 62%, and 64% of cases at 0.3, 1, and 2 s, respectively, and it was greater than 2 cmH2O, in 10%, 20%, and 15% of cases at 0.3, 1, and 2 s, respectively.
Conclusions: The pattern of Paw during an end-inspiratory occlusion in pressure support cannot assure the absence of expiratory muscle activity and accurate measurement of driving pressure. Yet, because driving pressure can only be overestimated due to expiratory muscle contraction, in everyday practice, a low driving pressure indicates an absence of global lung over-stretch. A measurement of high driving pressure should prompt further diagnostic workup, such as a measurement of esophageal pressure.
Keywords: Driving pressure; Esophageal pressure; Gastric pressure; Protective ventilation.
Conflict of interest statement
S.S. has no competing interests to declare. E.A., E.K., K.V., and D.G. have received lecture fees from Medtronic.
Figures
References
-
- Neto AS, Hemmes SNT, Barbas CSV, Beiderlinden M, Fernandez-Bustamante A, Futier E, et al. Association between driving pressure and development of postoperative pulmonary complications in patients undergoing mechanical ventilation for general anaesthesia: a meta-analysis of individual patient data. Lancet Respir Med. 2016;4:272–280. doi: 10.1016/S2213-2600(16)00057-6. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
