

Antihypertensive Deprescribing in Older Adult Veterans at End of Life Admitted to Veteran Affairs Nursing Homes
- PMID: 32723537
- PMCID: PMC7769911
- DOI: 10.1016/j.jamda.2020.05.060
Antihypertensive Deprescribing in Older Adult Veterans at End of Life Admitted to Veteran Affairs Nursing Homes
Erratum in
-
Erratum.J Am Med Dir Assoc. 2021 Sep;22(9):1966. doi: 10.1016/j.jamda.2021.06.002. Epub 2021 Jun 8. J Am Med Dir Assoc. 2021. PMID: 34115992 No abstract available.
Abstract
Objectives: Geriatric palliative care approaches support deprescribing of antihypertensives in older nursing home (NH) residents with limited life expectancy and/or advanced dementia (LLE/AD) who are intensely treated for hypertension (HTN), but information on real-world deprescribing patterns in this population is limited. We examined the incidence and factors associated with antihypertensive deprescribing.
Design: National, retrospective cohort study.
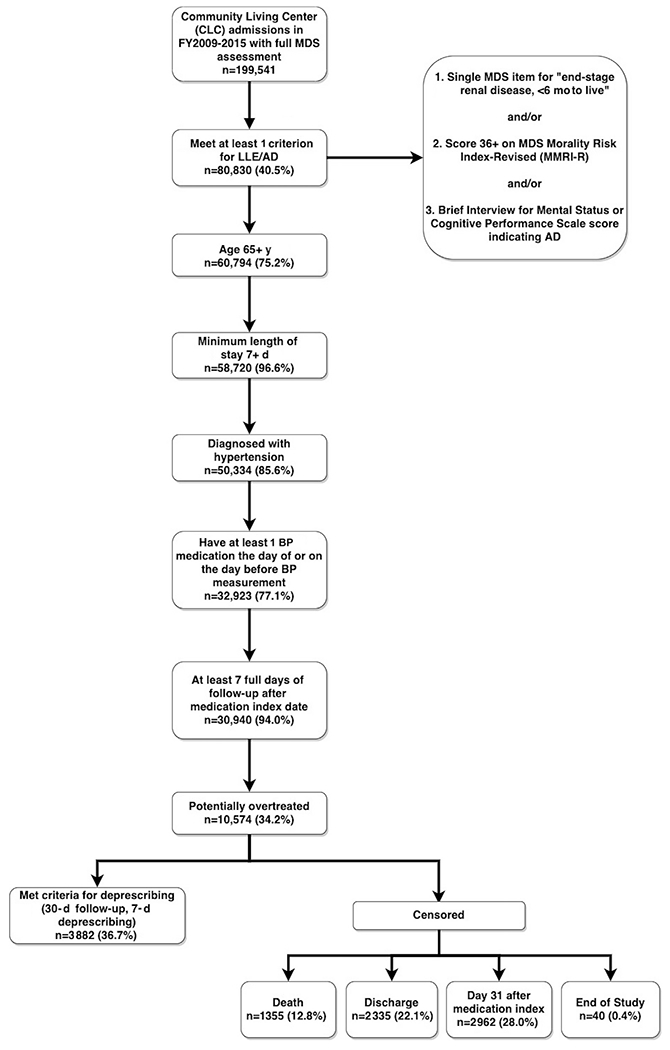
Setting and participants: Older Veterans with LLE/AD and HTN admitted to VA NHs in fiscal years 2009-2015 with potential overtreatment of HTN at admission, defined as receiving at least 1 antihypertensive class of medications and mean daily systolic blood pressure (SBP) <120 mm Hg.
Measures: Deprescribing was defined as subsequent dose reduction or discontinuation of an antihypertensive for ≥7 days. Competing risk models assessed cumulative incidence and factors associated with deprescribing.
Results: Within our sample (n = 10,574), cumulative incidence of deprescribing at 30 days was 41%. Veterans with the greatest level of overtreatment (ie, multiple antihypertensives and SBP <100 mm Hg) had an increased likelihood (hazard ratio 1.75, 95% confidence interval 1.59, 1.93) of deprescribing vs those with the lowest level of overtreatment (ie, one antihypertensive and SBP ≥100 to <120 mm Hg). Several markers of poor prognosis (ie, recent weight loss, poor appetite, dehydration, dependence for activities of daily living, pain) and later admission year were associated with increased likelihood of deprescribing, whereas cardiovascular risk factors (ie, diabetes, congestive heart failure, obesity), shortness of breath, and admission source from another NH or home/assisted living setting (vs acute hospital) were associated with decreased likelihood.
Conclusions and implications: Real-world deprescribing patterns of antihypertensives among NH residents with HTN and LLE/AD appear to reflect variation in recommendations for HTN treatment intensity and individualization of patient care in a population with potential overtreatment. Factors facilitating deprescribing included treatment intensity and markers of poor prognosis. Comparative effectiveness and safety studies are needed to guide clinical decisions around deprescribing and HTN management.
Keywords: Hypertension; antihypertensives; deprescribing; end-of-life; nursing homes; older adults.
Published by Elsevier Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Morin L, Vetrano DL, Rizzuto D, et al. Choosing wisely? Measuring the burden of medications in older adults near the end of life: Nationwide, longitudinal cohort study. Am J Med 2017;130:927–936.e9. - PubMed
-
- Scott IA, Hilmer SN, Reeve E, et al. Reducing inappropriate polypharmacy: The process of deprescribing. JAMA Intern Med 2015;175:827–834. - PubMed
-
- Todd A, Husband A, Andrew I, et al. Inappropriate prescribing of preventative medication in patients with life-limiting illness: A systematic review. BMJ Support Palliat Care 2017;7:113–121. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
