

Historical and projected hysterectomy rates in the USA: Implications for future observed cervical cancer rates and evaluating prevention interventions
- PMID: 32723676
- PMCID: PMC8723888
- DOI: 10.1016/j.ygyno.2020.05.030
Historical and projected hysterectomy rates in the USA: Implications for future observed cervical cancer rates and evaluating prevention interventions
Abstract
Background: SEER-reported cervical cancer incidence rates reflect the total female population including women no longer at risk due to hysterectomy. Hysterectomy rates have been declining in the United States as alternative treatments have become available, which could result in an apparent increase in SEER-reported cervical cancer rates. We aimed to obtain nationally representative historical data on hysterectomy rates in USA, use trends analysis to project rates back to 1935 and forward to 2035, and then predict the impact of changing hysterectomy rates on SEER-reported cervical cancer rates.
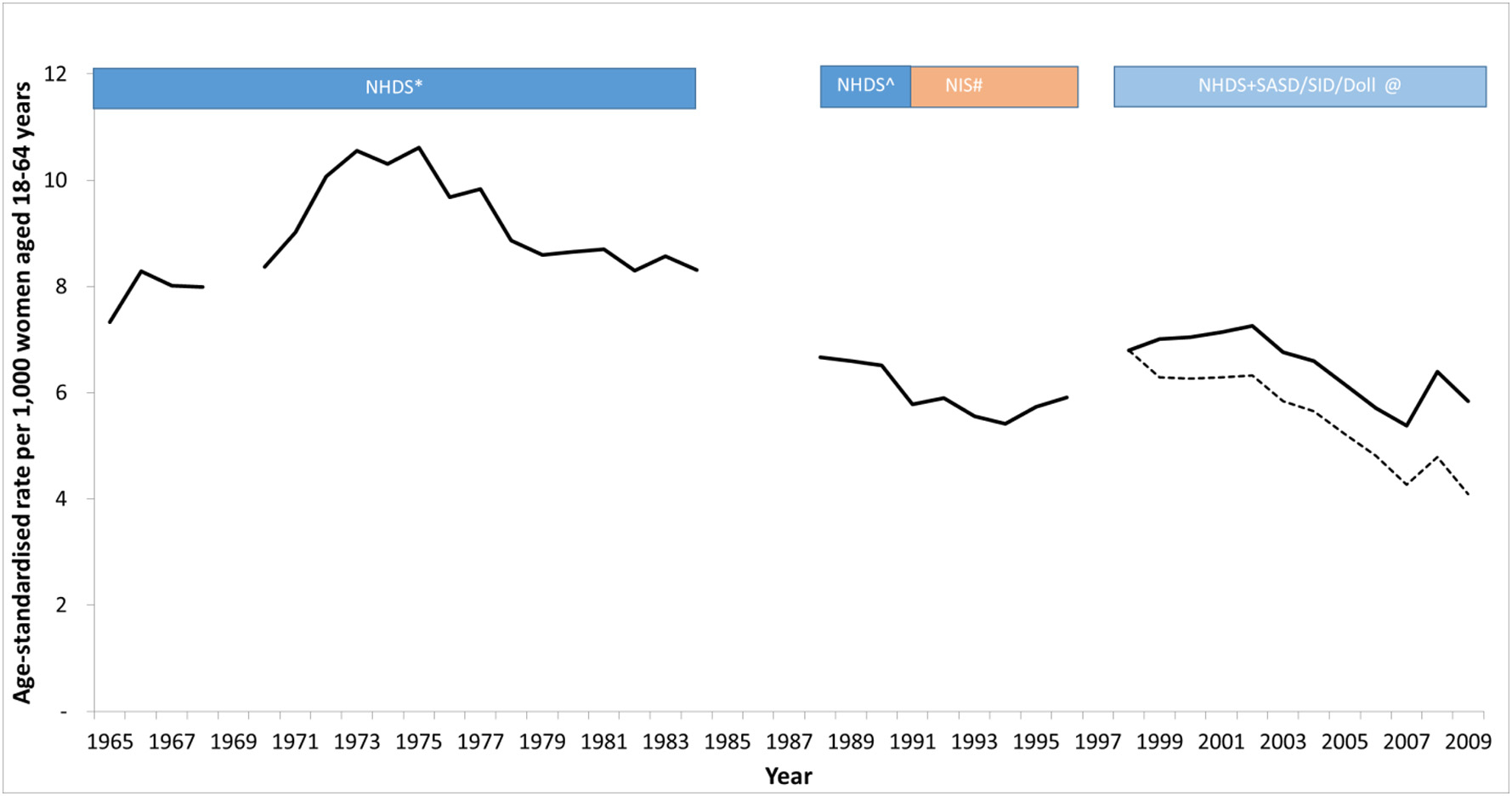
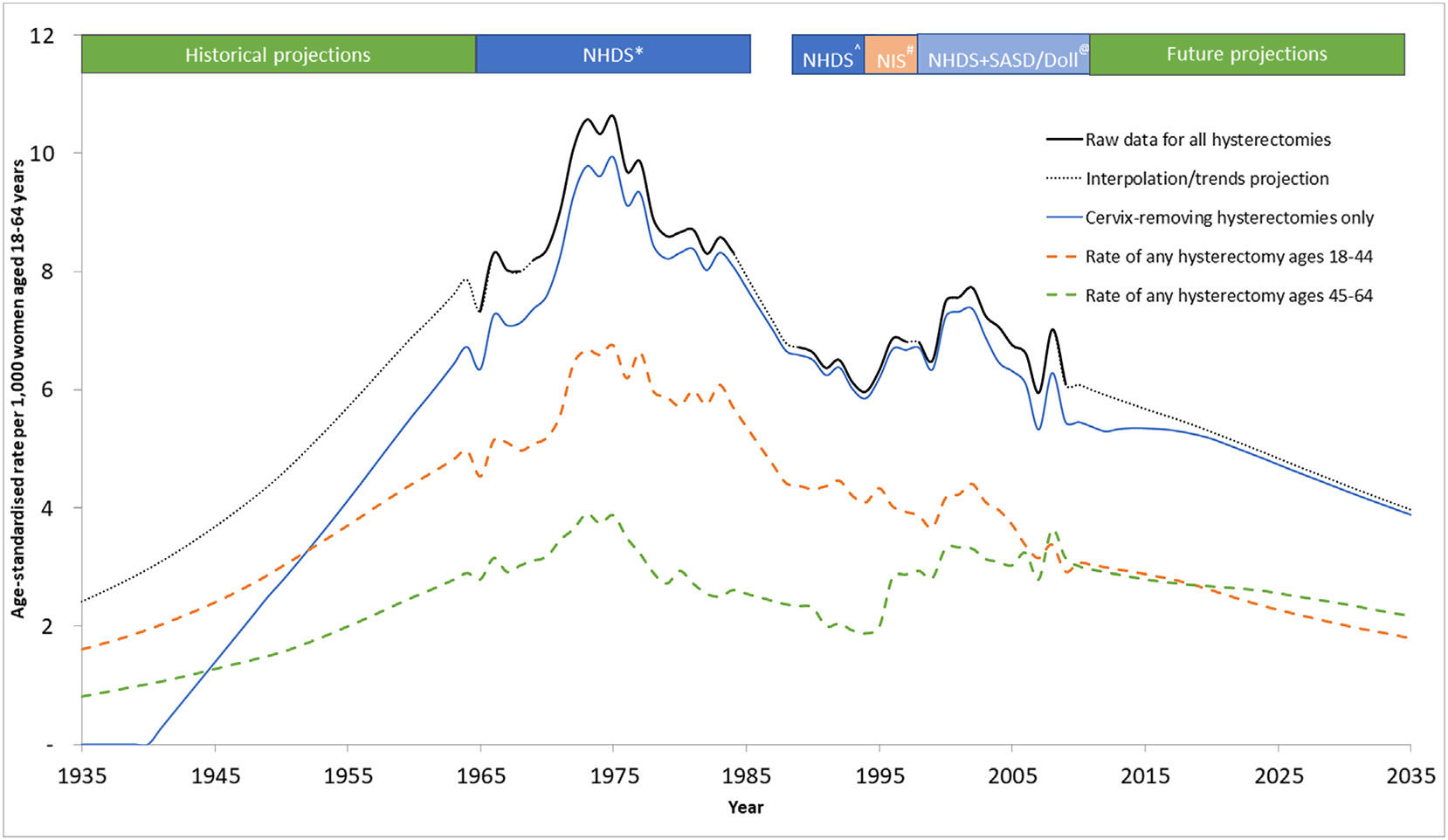
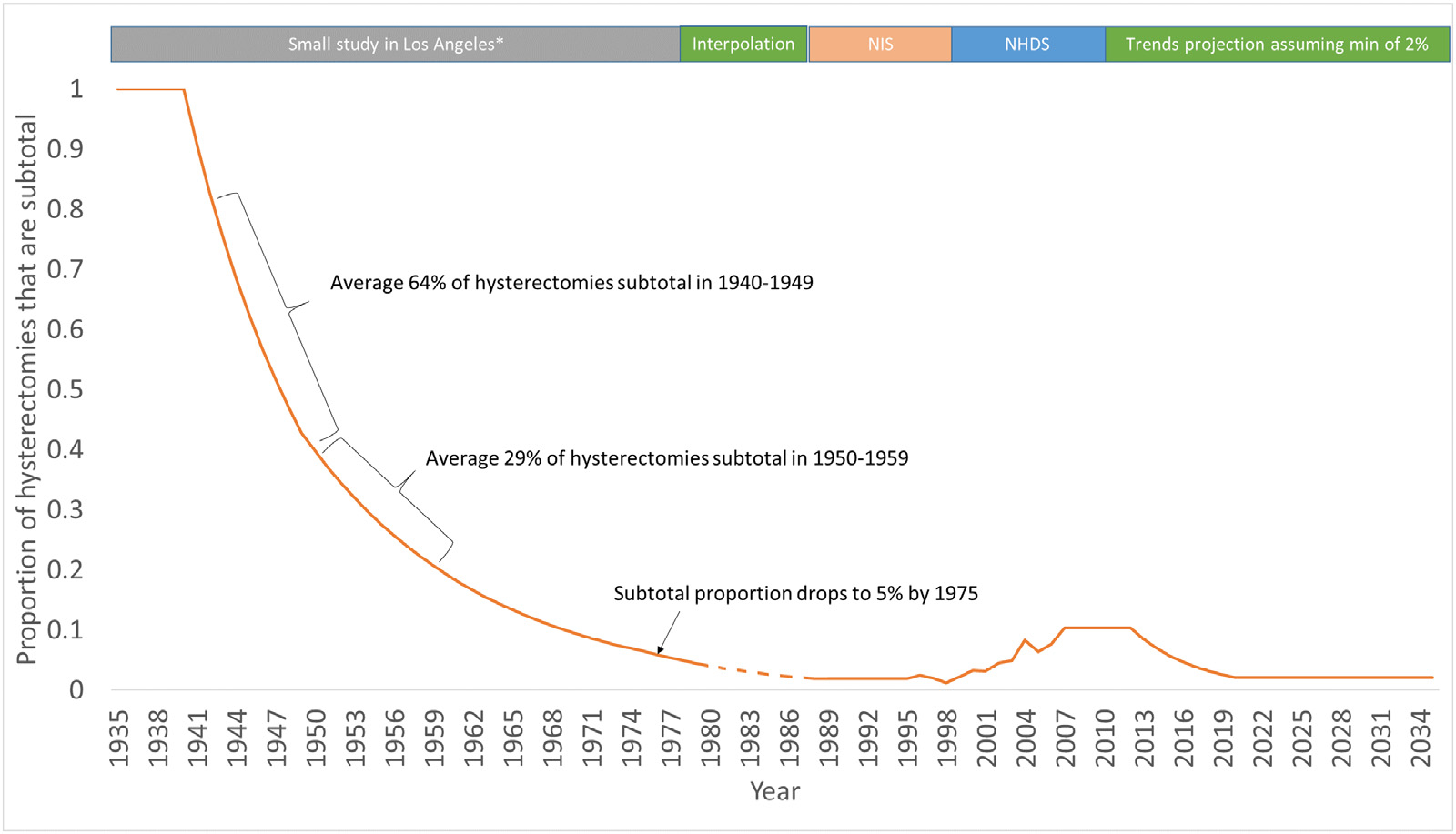
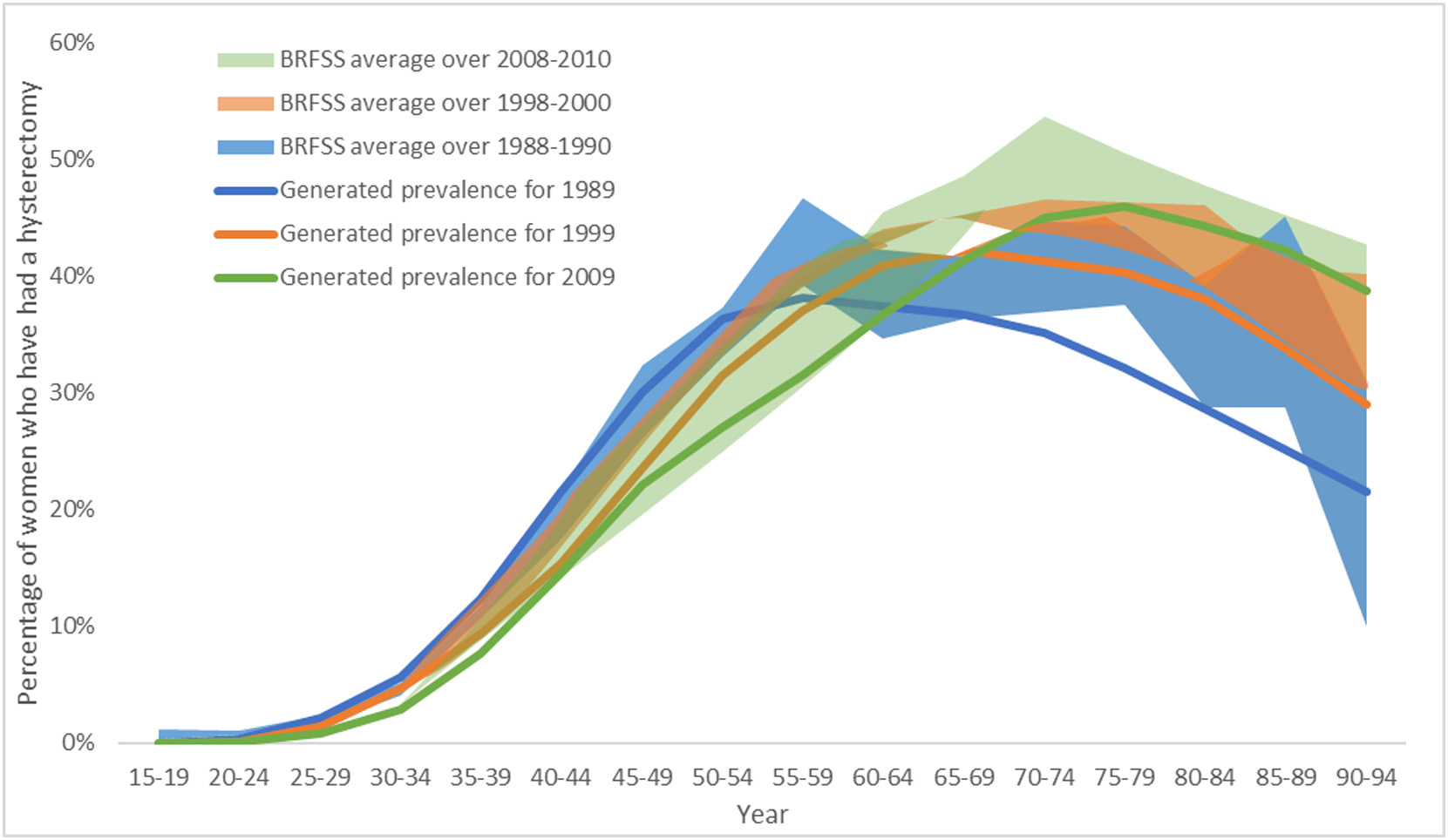
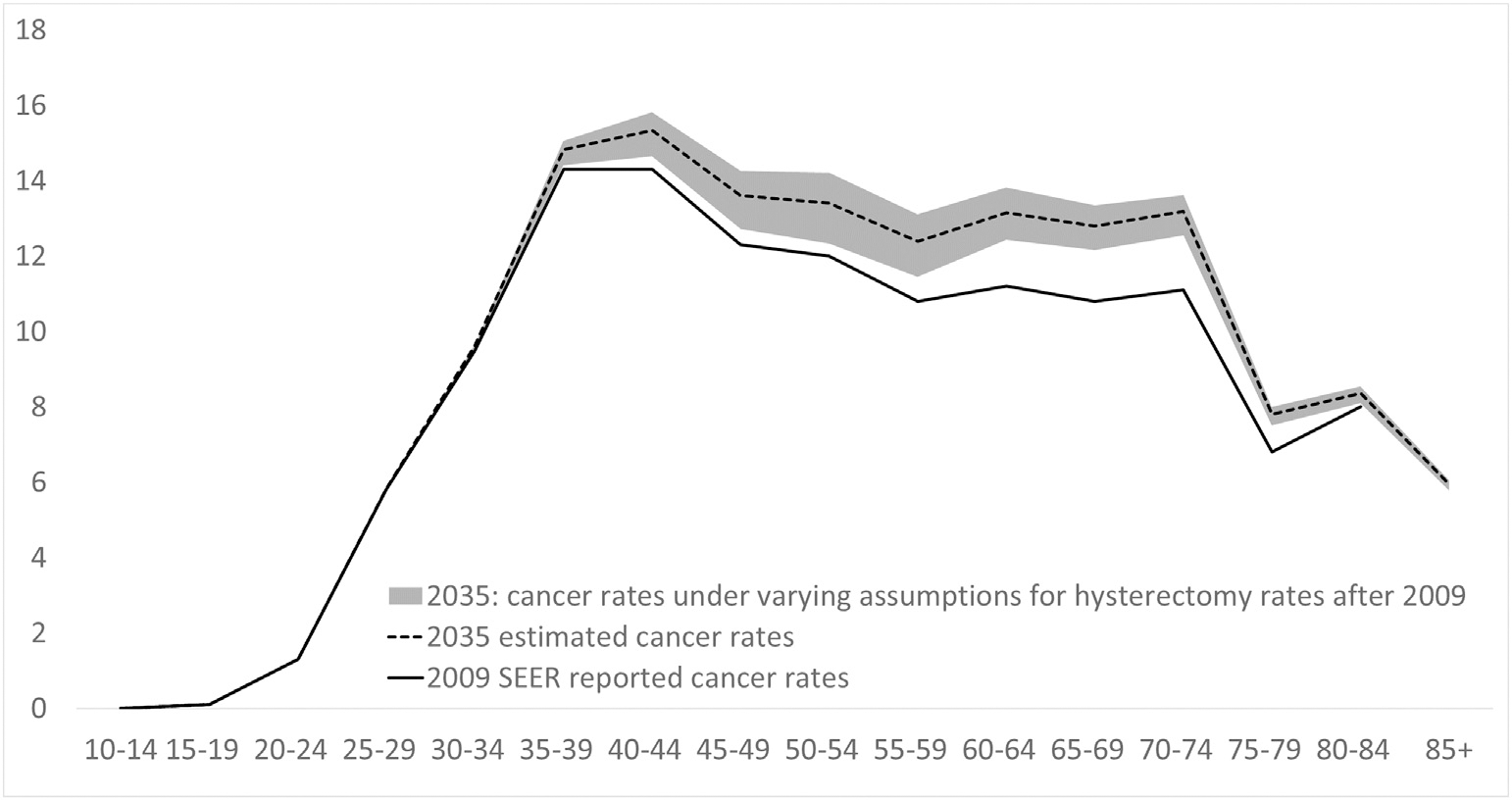
Methods: We performed a systematic search of Medline, Embase, Premedline, Cochrane Central databases and extracted nationally-representative hysterectomy incidence data from 1965 to 2009, including data on the number of cervix-preserving (subtotal) procedures. We then projected rates back to 1935, and forward to 2035 based on trends from joinpoint regression. These rates were then used to estimate hysterectomy prevalence out to 2035, and then to predict the impact of changing hysterectomy rates on SEER-reported cervical cancer rates to 2035. We examined alternative assumptions regarding projected hysterectomy incidence rates out to 2035, including a scenario in which rates decline no further from 2009 rates, and a scenario where rates decline at twice the baseline rate.
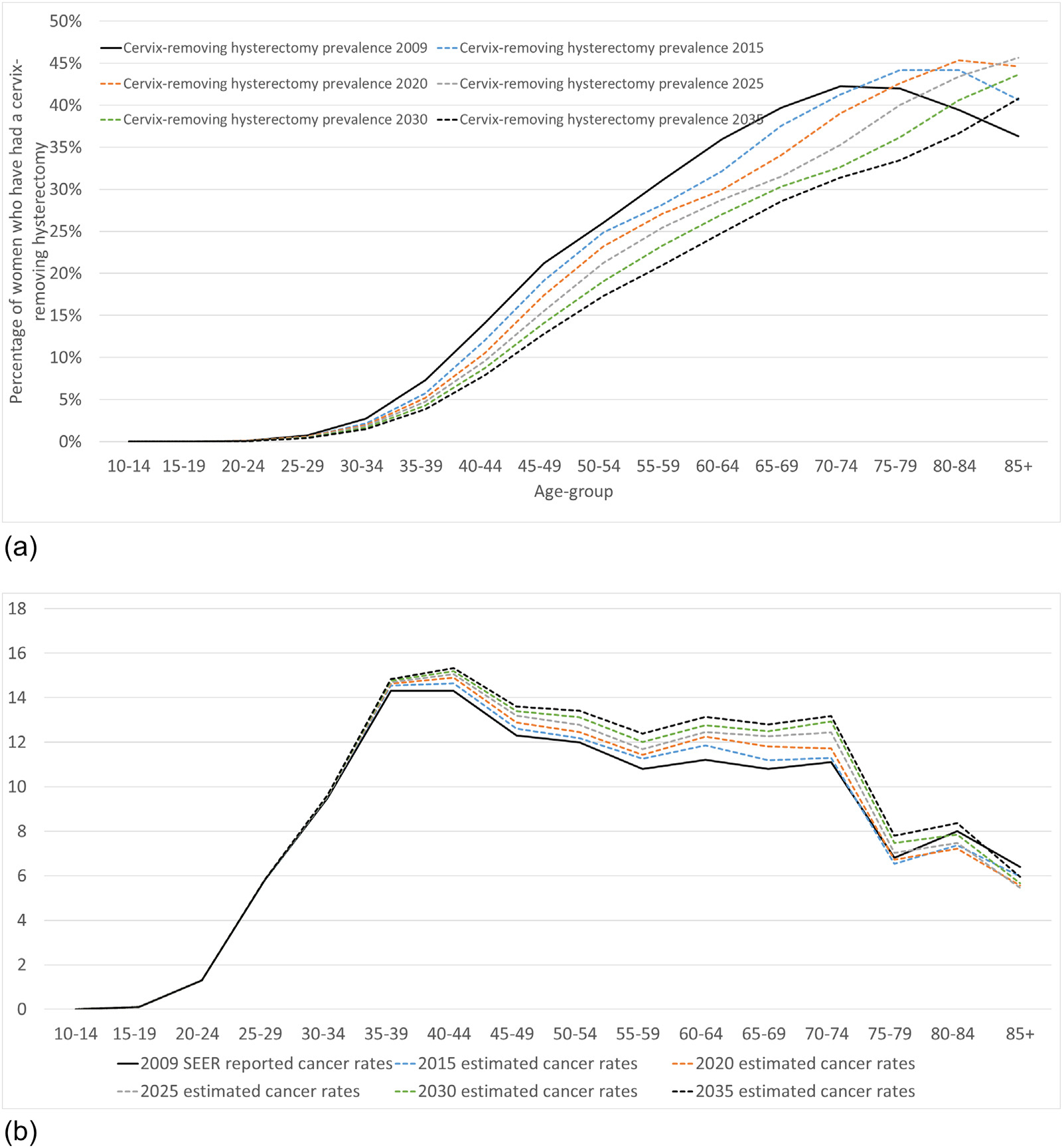
Results: Estimated age-standardized hysterectomy incidence increased from 2.4 to 10.6 per 1000 women between 1935 and 1975. Thereafter, rates are predicted to fall to 3.9 per 1000 by 2035. Subtotal hysterectomy procedures declined from being the predominant method in 1935 to less than 12% of procedures from 1970 onwards. Consequently, holding all else constant, an increase in SEER-reported age-standardized cervical cancer incidence rates (ages 0-85+) of 9% is expected from 2009 to 2035. The predictions were minimally impacted by alternative scenarios for future hysterectomy rates.
Conclusions: Declining hysterectomy rates have implications for the interpretation of SEER-reported cervical cancer rates. A background increase in cervical cancer rates due to decreasing population hysterectomy exposure may partially offset expected decreases from recent cervical screening changes recommended by the US Preventive Services Task Force. Evaluations of new cervical cancer prevention opportunities should consider the background impact of historical and projected hysterectomy rates.
Keywords: Cervical cancer; Hysterectomy; Trends; USA.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest KS receives salary support from the Cancer Institute. MAS receives salary support from the National Health and Medical Research Council (Australia) and the Cancer Institute NSW. KC is co-PI of an unrelated investigator-initiated trial of cytology and primary HPV screening in Australia (‘Compass’), which is conducted and funded by the VCS Foundation, a government-funded health promotion charity. In 2013, the VCS Foundation received equipment and a funding contribution for the Compass trial from Roche Molecular Systems and Ventana Inc. USA. However, neither KC nor her institution (Cancer Council NSW) receives direct funding from industry for this trial or any other project. All other authors declare no conflicts of interest.
Figures
References
-
- Agency for Healthcare Research and Quality R, MD, HCUP Nationwide Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP), https://www.hcupus.ahrq.gov/nisoverview.jsp. (Accessed 9 October 2017).
-
- Reich H, Decaprio J, McGlynn F, Laparoscopic hysterectomy J Gynecol. Surg. 5 (1989) 213–216.
-
- Farquhar CM, Steiner CA, Hysterectomy rates in the United States 1990–1997, Obstet. Gynecol. 99 (2) (2002) 229–234. - PubMed
-
- Wright JD, Ananth CV, Lewin SN, et al., Robotically assisted vs laparoscopic hysterectomy among women with benign gynecologic disease, Jama. 309 (7) (2013) 689–698. - PubMed
