

Developments in the Histopathological Classification of ANCA-Associated Glomerulonephritis
- PMID: 32723805
- PMCID: PMC7409752
- DOI: 10.2215/CJN.14561119
Developments in the Histopathological Classification of ANCA-Associated Glomerulonephritis
Abstract
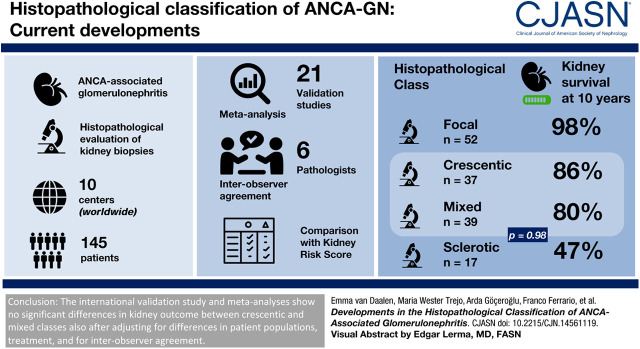
Background and objectives: The histopathologic classification for ANCA-associated GN distinguishes four classes on the basis of patterns of injury. In the original validation study, these classes were ordered by severity of kidney function loss as follows: focal, crescentic, mixed, and sclerotic. Subsequent validation studies disagreed on outcomes in the crescentic and mixed classes. This study, driven by the original investigators, provides several analyses in order to determine the current position of the histopathologic classification of ANCA-associated GN.
Design, setting, participants, & measurements: A validation study was performed with newly collected data from 145 patients from ten centers worldwide, including an analysis of interobserver agreement on the histopathologic evaluation of the kidney biopsies. This study also included a meta-analysis on previous validation studies and a validation of the recently proposed ANCA kidney risk score.
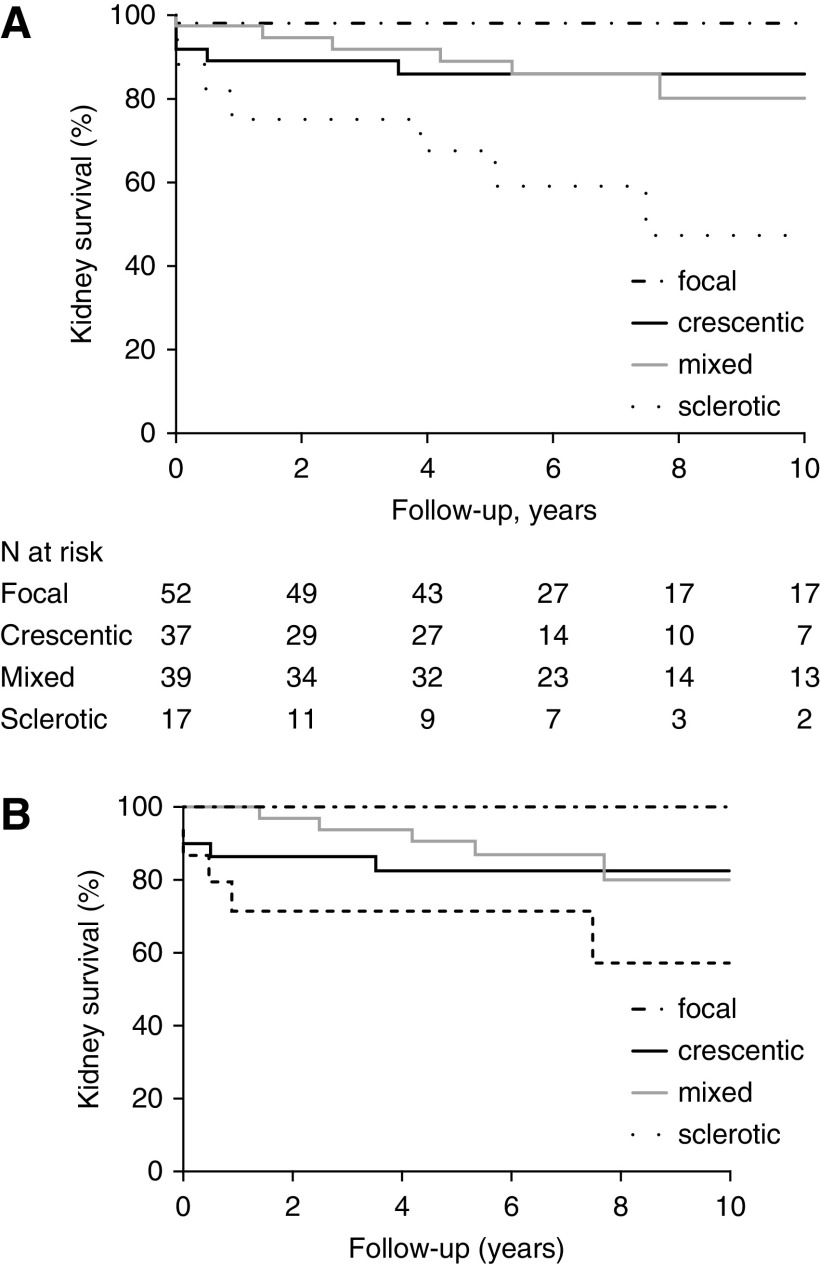
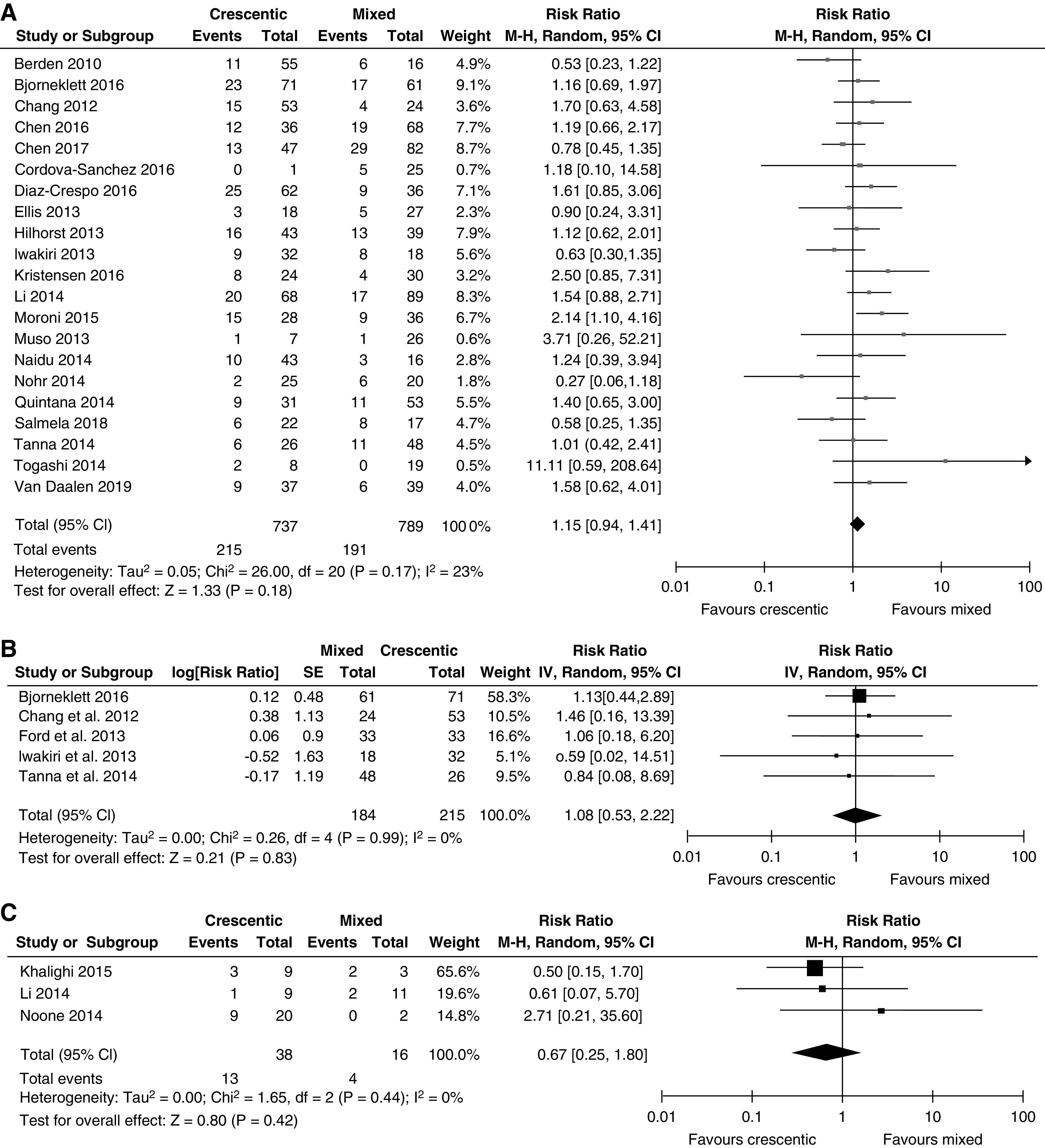
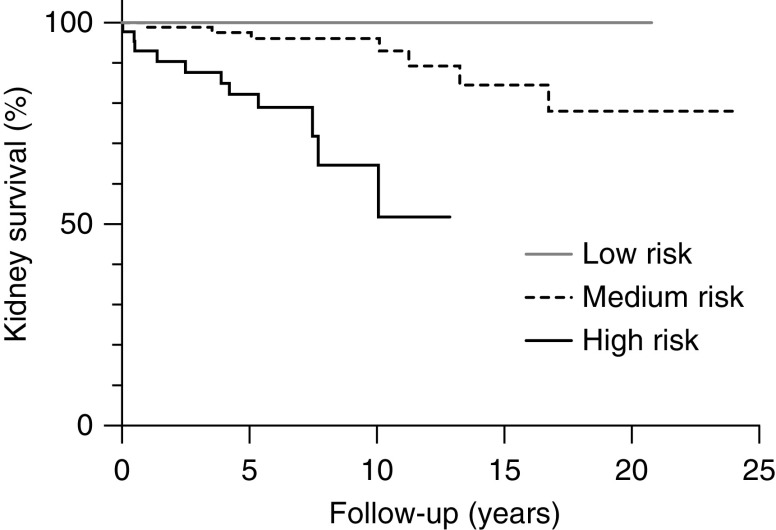
Results: The validation study showed that kidney failure at 10-year follow-up was significantly different between the histopathologic classes (P<0.001). Kidney failure at 10-year follow-up was 14% in the crescentic class versus 20% in the mixed class (P=0.98). In the meta-analysis, no significant difference in kidney failure was also observed when crescentic class was compared with mixed class (relative risk, 1.15; 95% confidence interval, 0.94 to 1.41). When we applied the ANCA kidney risk score to our cohort, kidney survival at 3 years was 100%, 96%, and 77% in the low-, medium-, and high-risk groups, respectively (P<0.001). These survival percentages are higher compared with the percentages in the original study.
Conclusions: The crescentic and mixed classes seem to have a similar prognosis, also after adjusting for differences in patient populations, treatment, and interobserver agreement. However, at this stage, we are not inclined to merge the crescentic and mixed classes because the reported confidence intervals do not exclude important differences in prognosis and because an important histopathologic distinction would be lost.
Keywords: ANCA; Antibodies; Antineutrophil Cytoplasmic; Biopsy; Cohort Studies; Confidence Intervals; Observer Variation; Prognosis; Renal Insufficiency; glomerulonephritis; kidney biopsy.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Keeping Up with the Times: Prognostic Tools in ANCA-Associated Glomerulonephritis.Clin J Am Soc Nephrol. 2020 Aug 7;15(8):1078-1080. doi: 10.2215/CJN.09600620. Epub 2020 Jul 28. Clin J Am Soc Nephrol. 2020. PMID: 32723806 Free PMC article. No abstract available.
References
-
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA: 2012 Revised International Chapel Hill Consensus Conference nomenclature of vasculitides. Arthritis Rheum 65: 1–11, 2013. - PubMed
-
- Hauer HA, Bajema IM, Van Houwelingen HC, Ferrario F, Noël LH, Waldherr R, Jayne DR, Rasmussen N, Bruijn JA, Hagen EC; European Vasculitis Study Group (EUVAS) : Determinants of outcome in ANCA-associated glomerulonephritis: A prospective clinico-histopathological analysis of 96 patients. Kidney Int 62: 1732–1742, 2002. - PubMed
-
- de Lind van Wijngaarden RA, Hauer HA, Wolterbeek R, Jayne DR, Gaskin G, Rasmussen N, Noël LH, Ferrario F, Waldherr R, Hagen EC, Bruijn JA, Bajema IM: Clinical and histologic determinants of renal outcome in ANCA-associated vasculitis: A prospective analysis of 100 patients with severe renal involvement. J Am Soc Nephrol 17: 2264–2274, 2006. - PubMed
-
- Bajema IM, Hagen EC, Hermans J, Noël LH, Waldherr R, Ferrario F, Van Der Woude FJ, Bruijn JA: Kidney biopsy as a predictor for renal outcome in ANCA-associated necrotizing glomerulonephritis. Kidney Int 56: 1751–1758, 1999. - PubMed
-
- Aasarød K, Bostad L, Hammerstrøm J, Jørstad S, Iversen BM: Renal histopathology and clinical course in 94 patients with Wegener’s granulomatosis. Nephrol Dial Transplant 16: 953–960, 2001. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
