

Coordinated Circulating T Follicular Helper and Activated B Cell Responses Underlie the Onset of Antibody-Mediated Rejection in Kidney Transplantation
- PMID: 32723838
- PMCID: PMC7608995
- DOI: 10.1681/ASN.2020030320
Coordinated Circulating T Follicular Helper and Activated B Cell Responses Underlie the Onset of Antibody-Mediated Rejection in Kidney Transplantation
Abstract
Background: Although antibody-mediated rejection (ABMR) has been long recognized as a leading cause of allograft failure after kidney transplantation, the cellular and molecular processes underlying the induction of deleterious donor-specific antibody (DSA) responses remain poorly understood.
Methods: Using high-dimensional flow cytometry, in vitro assays, and RNA sequencing, we concomitantly investigated the role of T follicular helper (TFH) cells and B cells during ABMR in 105 kidney transplant recipients.
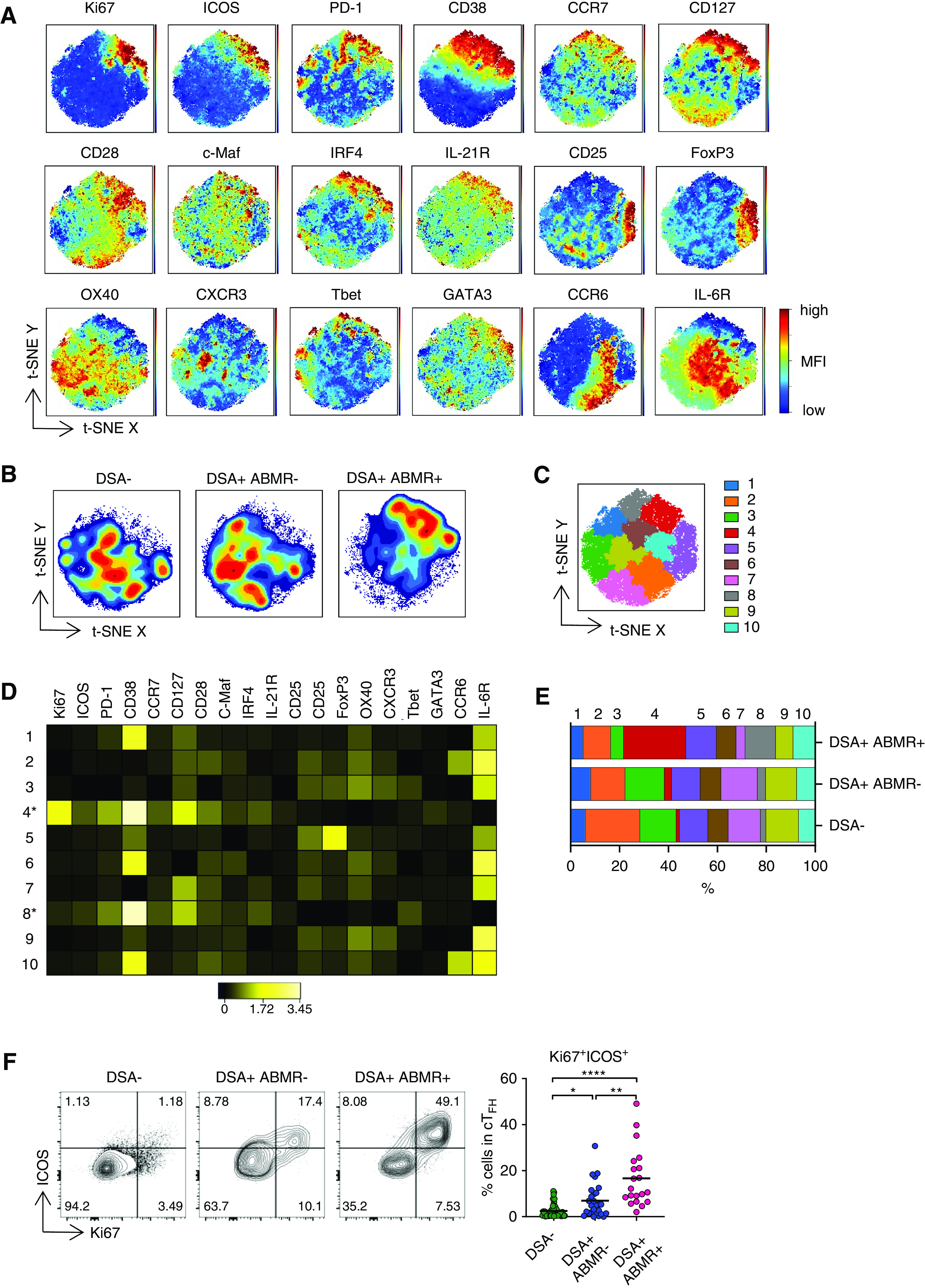
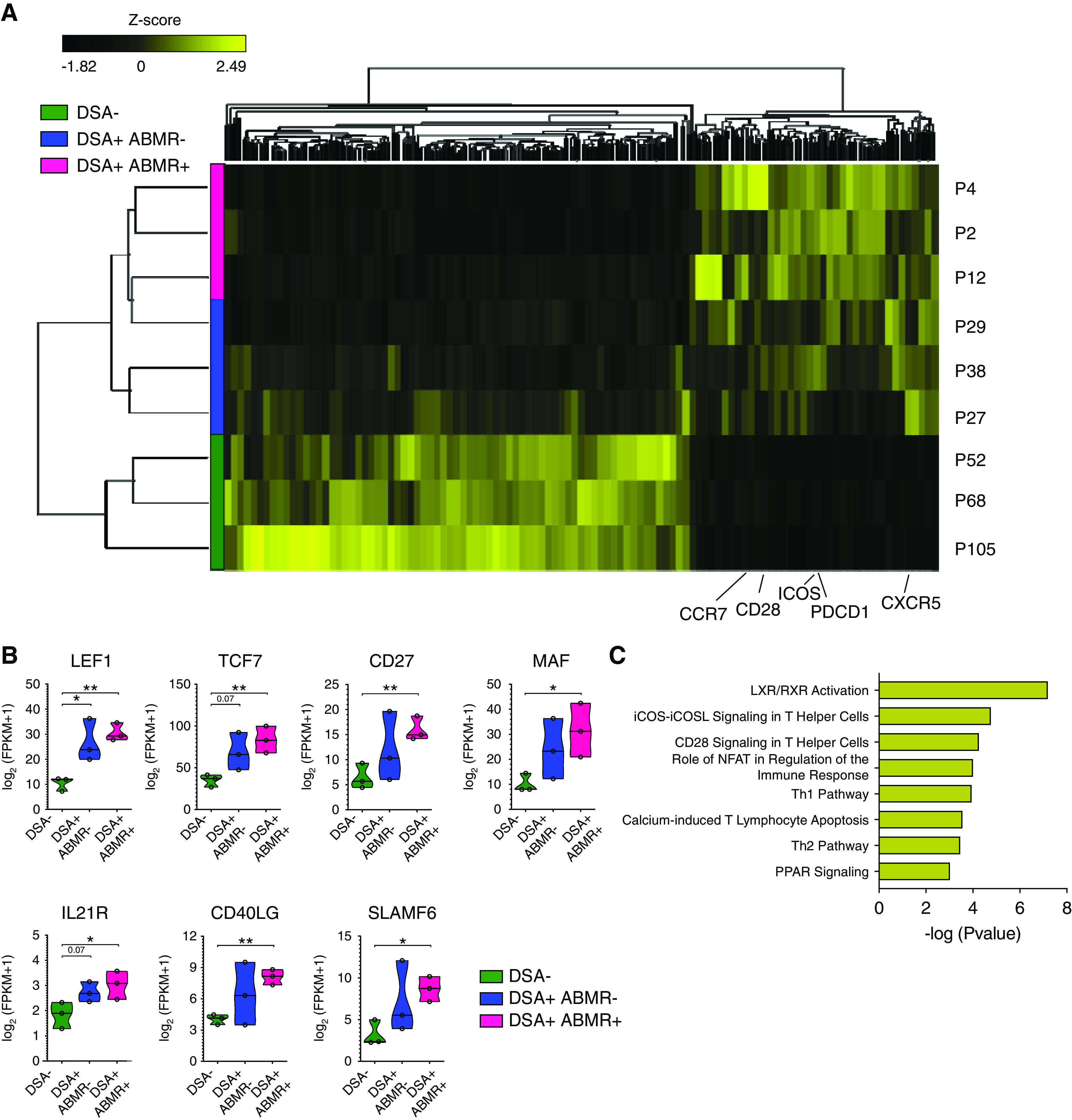
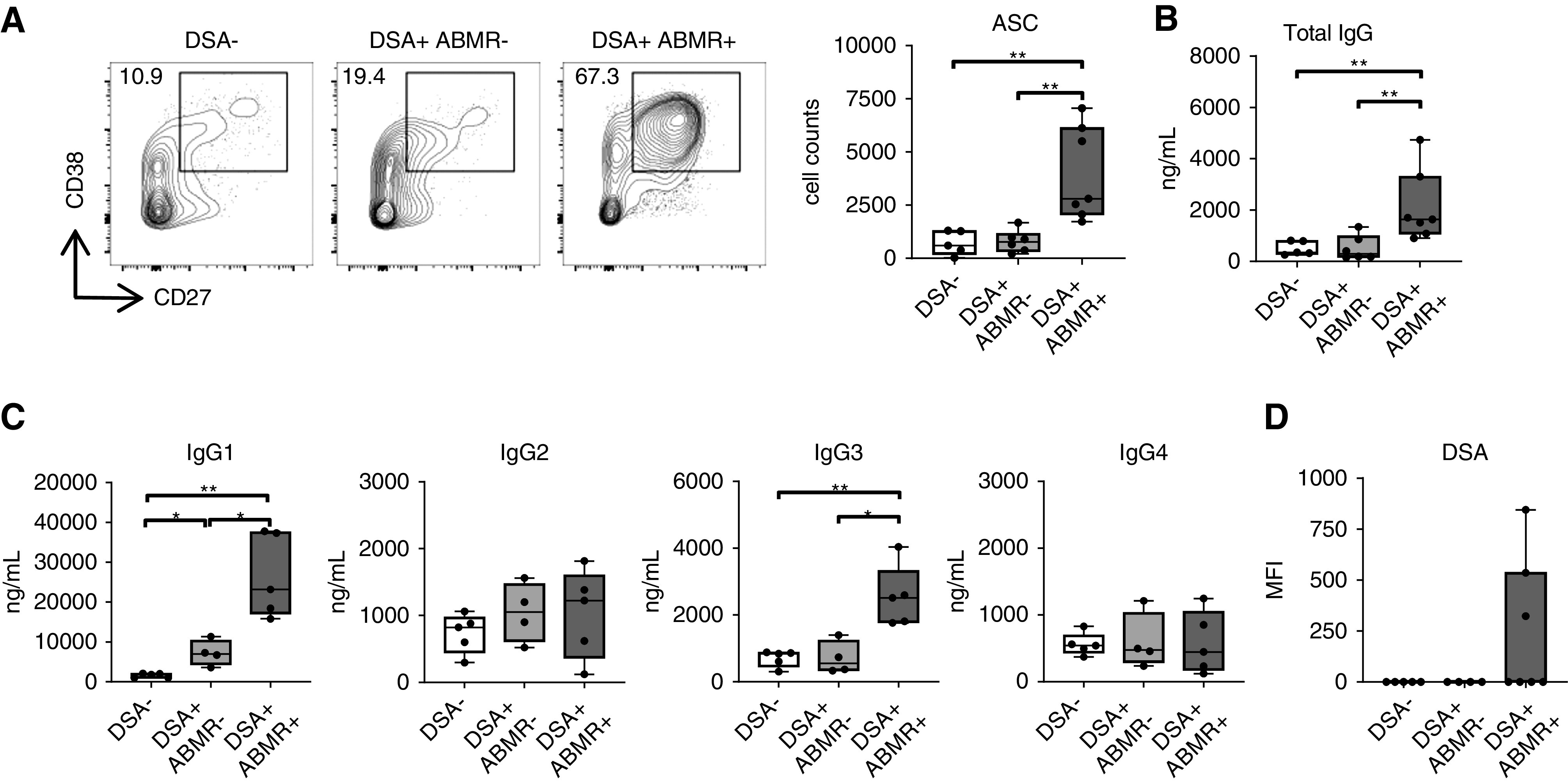
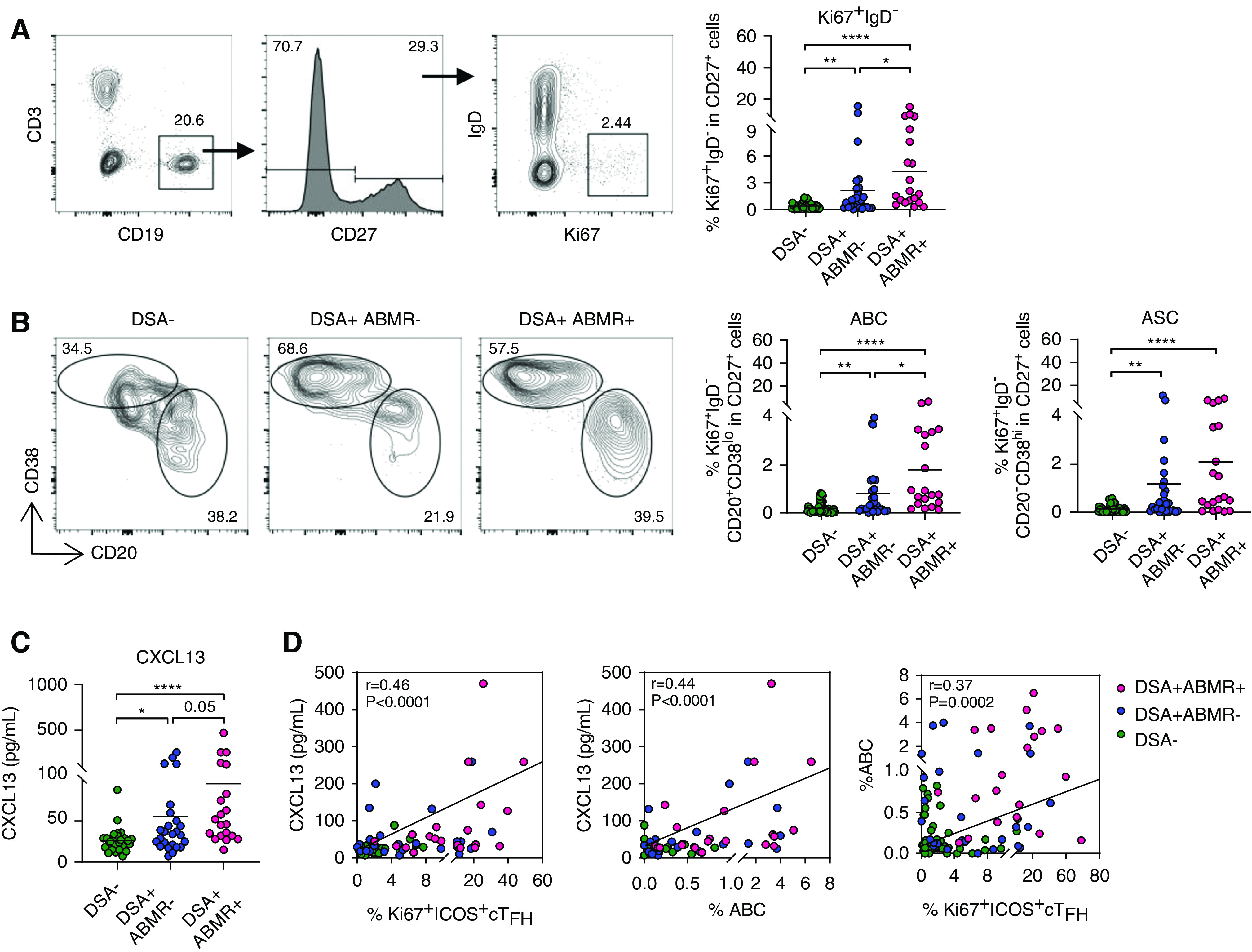
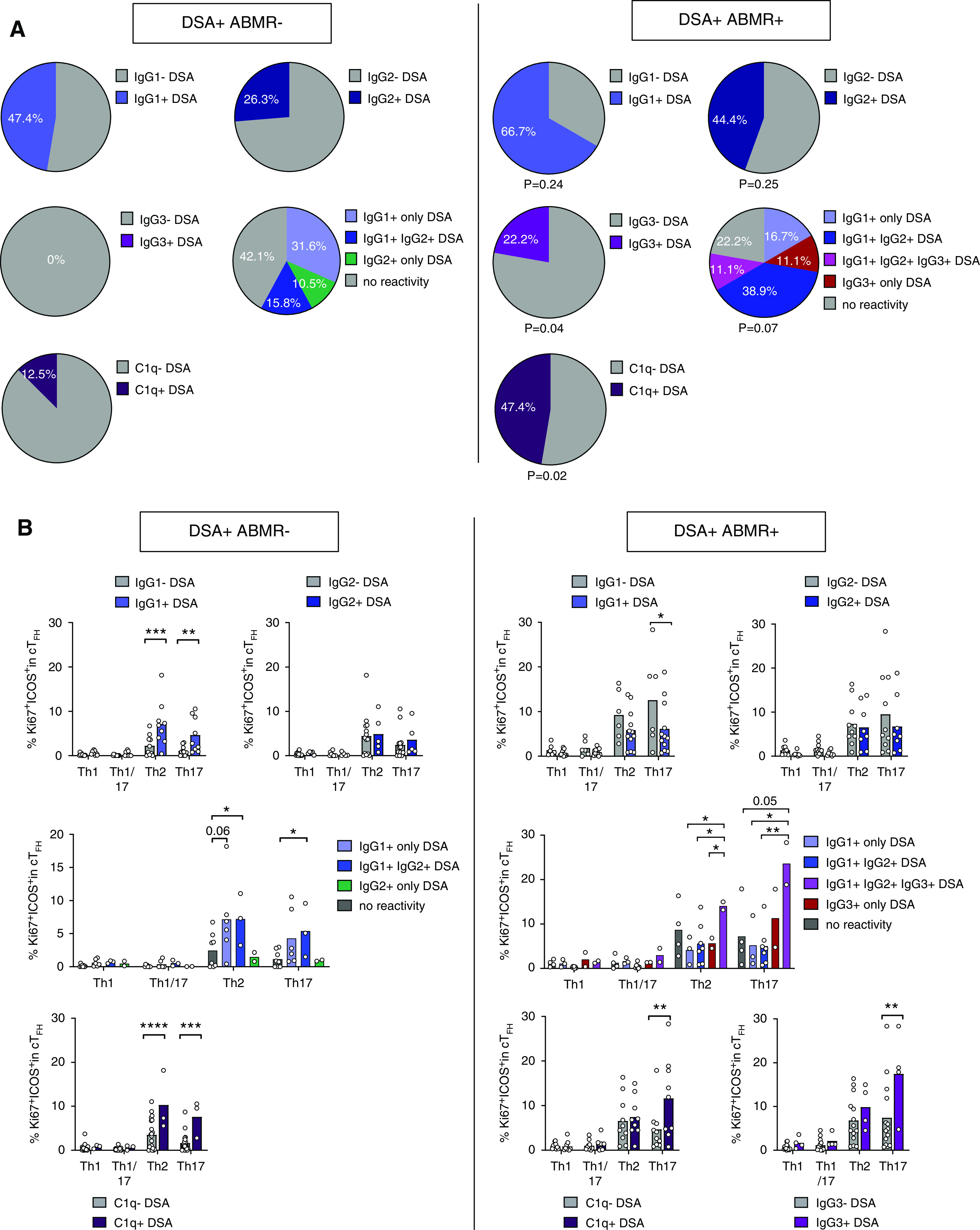
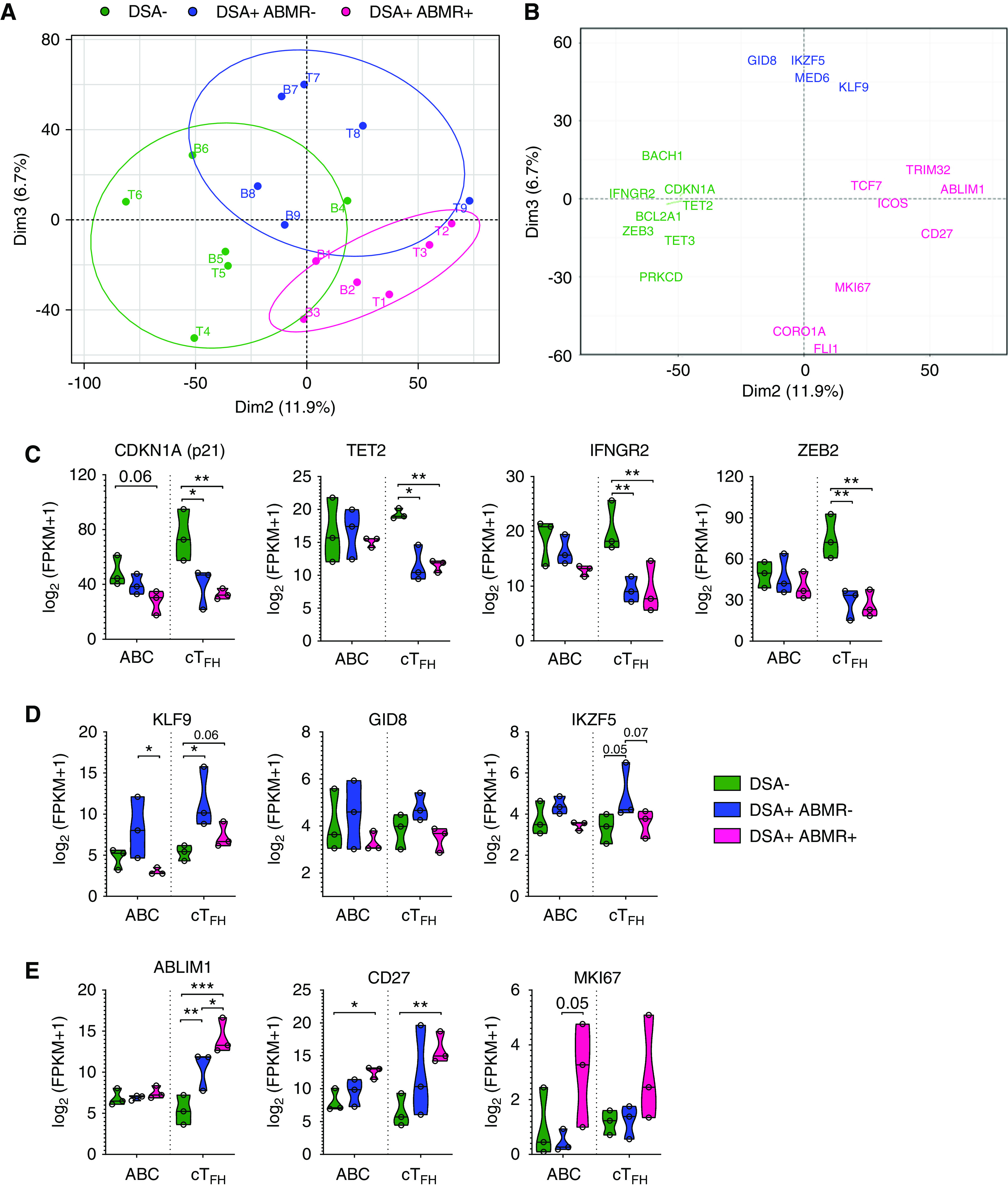
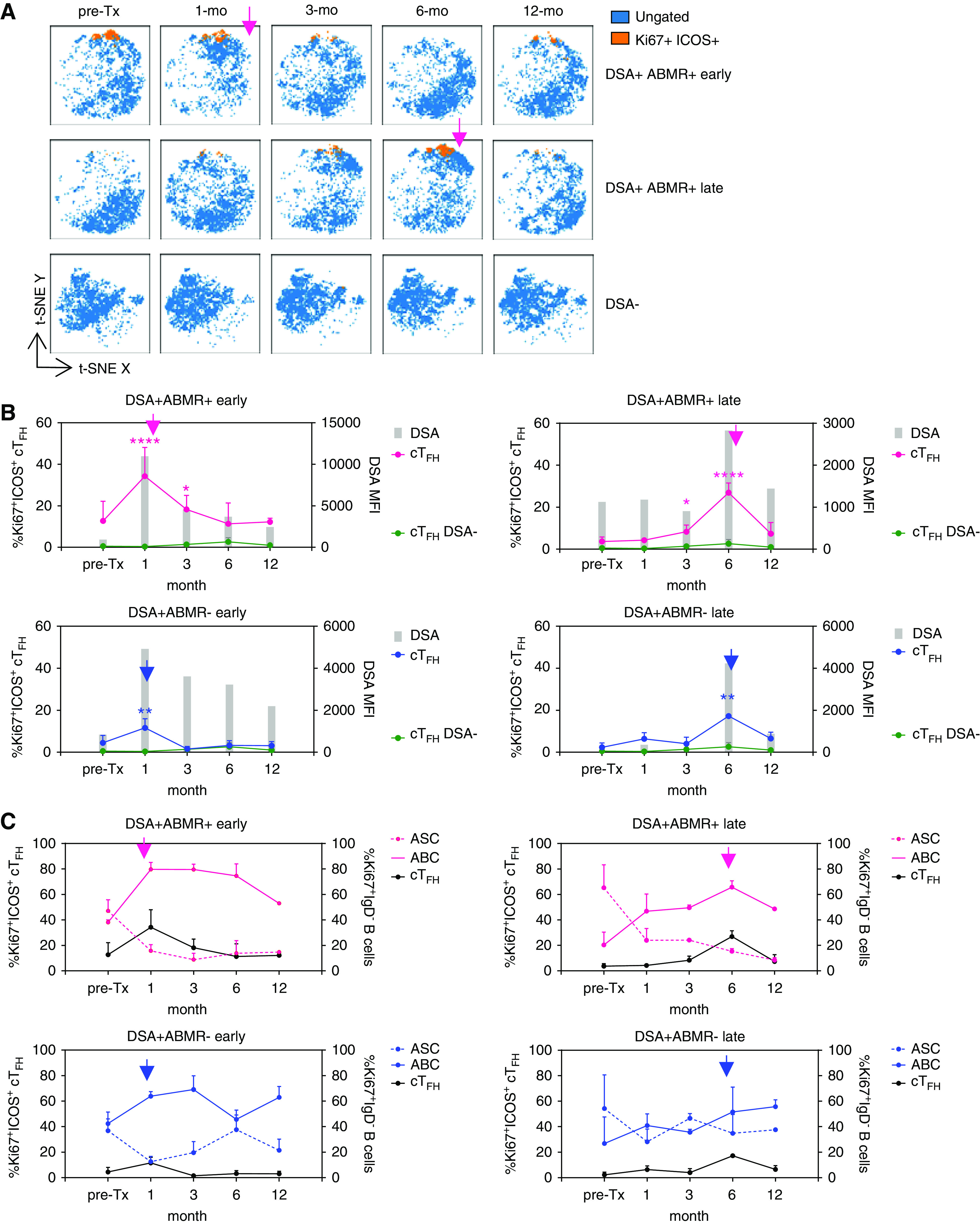
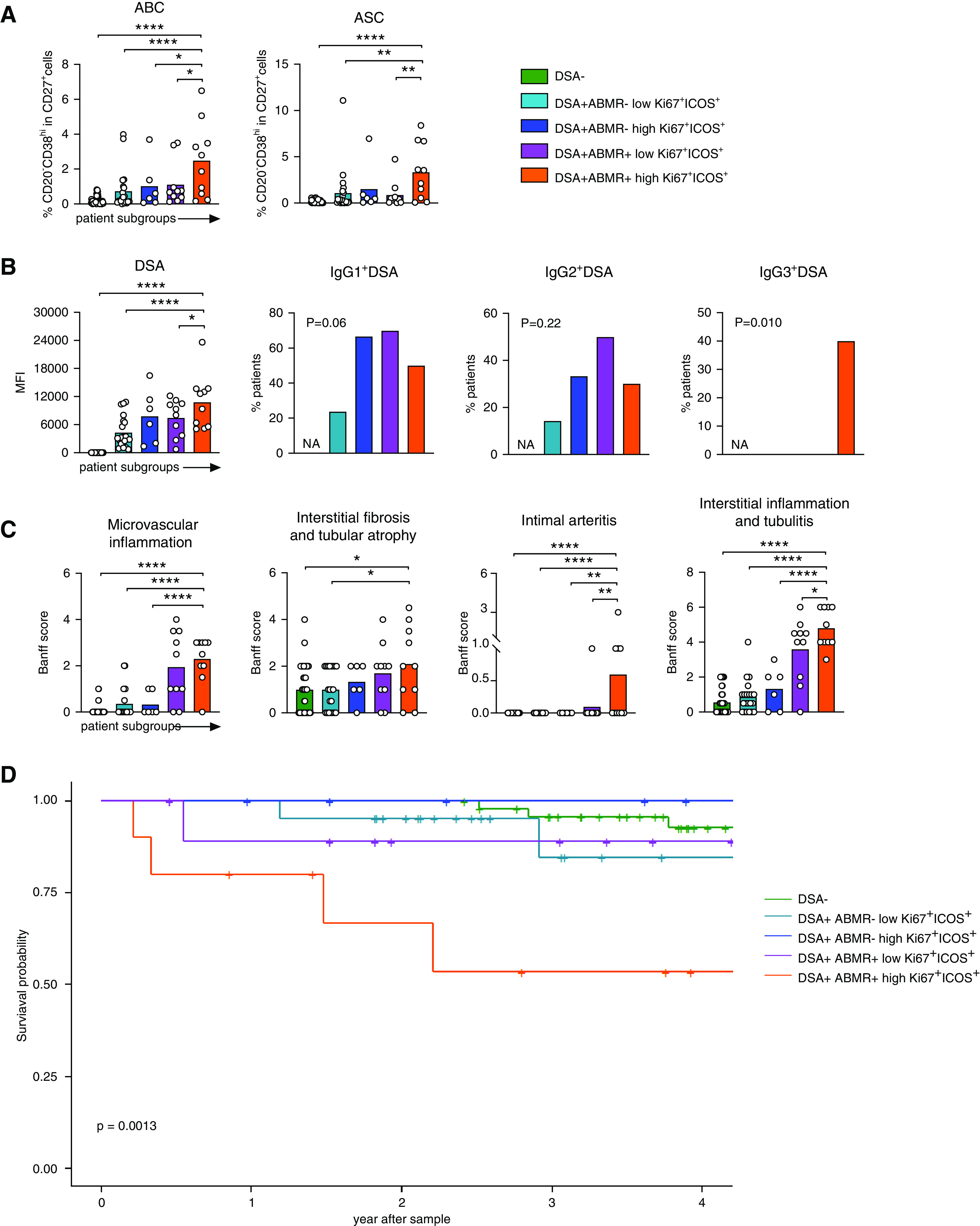
Results: There were 54 patients without DSAs; of those with DSAs, ABMR emerged in 20 patients, but not in 31 patients. We identified proliferating populations of circulating TFH cells and activated B cells emerging in blood of patients undergoing ABMR. Although these circulating TFH cells comprised heterogeneous phenotypes, they were dominated by activated (ICOS+PD-1+) and early memory precursor (CCR7+CD127+) subsets, and were enriched for the transcription factors IRF4 and c-Maf. These circulating TFH cells produced large amounts of IL-21 upon stimulation with donor antigen and induced B cells to differentiate into antibody-secreting cells that produced DSAs. Combined analysis of the matched circulating TFH cell and activated B cell RNA-sequencing profiles identified highly coordinated transcriptional programs in circulating TFH cells and B cells among patients with ABMR, which markedly differed from those of patients who did not develop DSAs or ABMR. The timing of expansion of the distinctive circulating TFH cells and activated B cells paralleled emergence of DSAs in blood, and their magnitude was predictive of IgG3 DSA generation, more severe allograft injury, and higher rate of allograft loss.
Conclusions: Patients undergoing ABMR may benefit from monitoring and therapeutic targeting of TFH cell-B cell interactions.
Keywords: acute allograft rejection; immunology; kidney transplantation; lymphocytes; transcriptional profiling; transplant outcomes.
Copyright © 2020 by the American Society of Nephrology.
Figures
References
-
- Loupy A, Lefaucheur C: Antibody-mediated rejection of solid-organ allografts. N Engl J Med 379: 1150–1160, 2018. - PubMed
-
- Louis K, Hertig A, Taupin J-L, Buob D, Jamme M, Brocheriou I, et al. .: Markers of graft microvascular endothelial injury may identify harmful donor-specific anti-HLA antibodies and predict kidney allograft loss. Am J Transplant 19: 2434–2445, 2019. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
