

Association of Maternal Opioid Use in Pregnancy With Adverse Perinatal Outcomes in Ontario, Canada, From 2012 to 2018
- PMID: 32725246
- PMCID: PMC12064095
- DOI: 10.1001/jamanetworkopen.2020.8256
Association of Maternal Opioid Use in Pregnancy With Adverse Perinatal Outcomes in Ontario, Canada, From 2012 to 2018
Abstract
Importance: A recent epidemic of opioid abuse has been described in many communities, although population-based data on trends in use in pregnancy and perinatal outcomes after in utero exposure remain limited.
Objective: To assess trends in prenatal opioid use and the potential association between prenatal opioid use and preterm birth and adverse perinatal outcomes.
Design, setting, and participants: This population-based retrospective cohort study covered live births and stillbirths among adolescents and women 15 years and older from April 1, 2012, to March 31, 2018, in Ontario, Canada. Data were analyzed from July 29 to October 15, 2019.
Exposures: Any opioid use in pregnancy, ascertained through self-reporting and routine prenatal care.
Main outcome and measures: The primary outcome was preterm birth before a gestational age of 37 weeks. Separate indicators for birth occurring at gestational ages of 34 to 36 weeks (plus 6 to 7 days; late preterm), 32 to 33 weeks (plus 6 to 7 days), 28 to 31 weeks (plus 6 to 7 days), and less than 28 weeks (very preterm birth). Secondary outcomes included small for gestational age, stillbirth, transfer to neonatal intensive care, and 5-minute Apgar score. Coarsened exact matching techniques and Poisson regression models were used to estimate the risk difference and relative risk (RR) of outcomes associated with cannabis exposure to control for confounding.
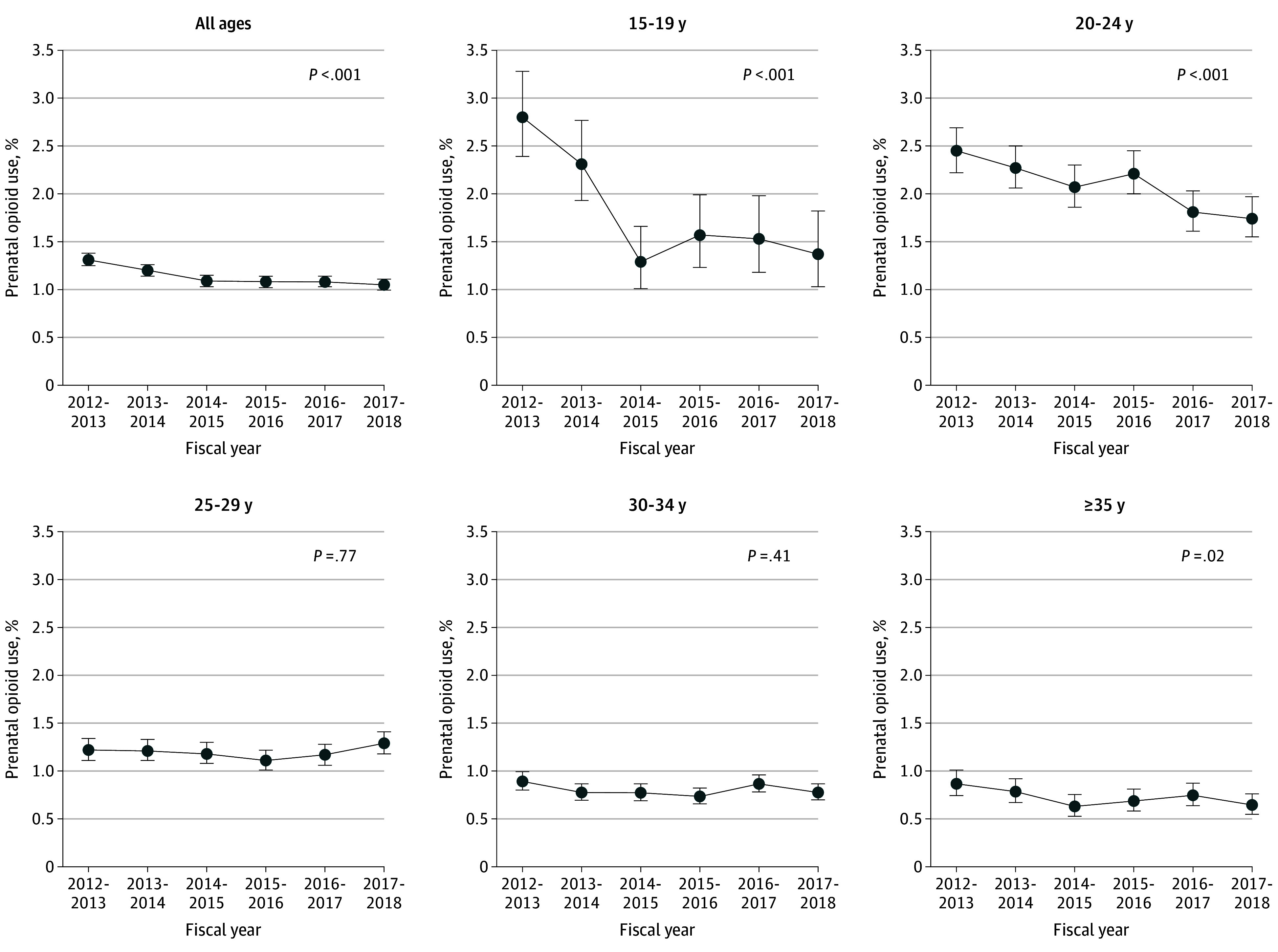
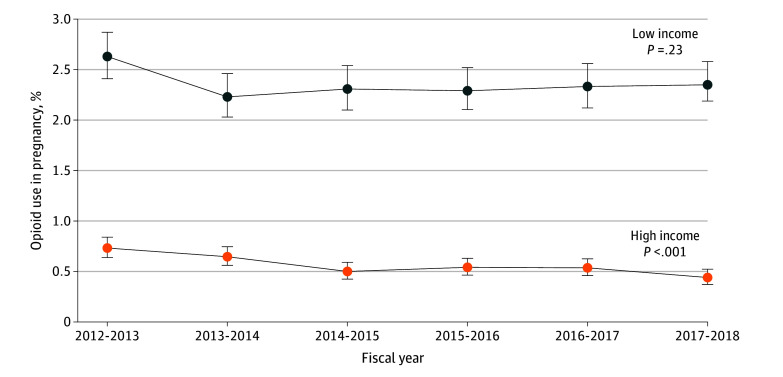
Results: Among 710 911 women included in the analytic sample (mean [SD] age, 30.4 [5.3] years), 8059 used opioids (1.1%), with prevalence decreasing from 1.31% (95% CI, 1.25%-1.38%) in fiscal year 2012-2013 to 1.05% (95% CI, 0.99%-1.11%) in fiscal year 2017-2018 (P < .001 for trend). Use was highest among women in the lowest quintile of area-level income (2.36% vs 0.56% in the highest quintile; RR, 3.86; 95% CI, 3.58-4.15) and did not decrease over time in this group (from 2.63% [95% CI, 2.41%-2.87%] in 2012-2013 to 2.35% [95% CI, 2.14%-2.58%] in 2017-2018; P = .23 for trend). The crude rate of preterm birth at a gestational age of less than 37 weeks was 14.0% (n = 1127) among women with reported use in pregnancy and 6.0% (n = 42 226) among women who did not use opioids in the unmatched cohort. The adjusted RR for preterm birth before a gestational age of 37 weeks was 1.63 (95% CI, 1.52-1.75) among opioid users compared with nonusers and 1.77 (95% CI, 1.35-2.31) for preterm birth before 32 weeks. Among newborns, risk for neonatal intensive care was 40.5% with perinatal exposure to opioids compared with 13.9% in unexposed infants (RR, 2.91; 95% CI, 2.80-3.03).
Conclusions and relevance: Rates of opioid use in pregnancy have declined in recent years, although use remains significantly higher among lower-income women. In this large population-based cohort, opioid use in pregnancy was associated with an increased risk of preterm birth and admission to a neonatal intensive care unit.
Conflict of interest statement
Figures
Similar articles
-
Association Between Self-reported Prenatal Cannabis Use and Maternal, Perinatal, and Neonatal Outcomes.JAMA. 2019 Jul 9;322(2):145-152. doi: 10.1001/jama.2019.8734. JAMA. 2019. PMID: 31211826 Free PMC article.
-
Obstetric and perinatal health outcomes after pertussis vaccination during pregnancy in Ontario, Canada: a retrospective cohort study.CMAJ Open. 2021 Apr 13;9(2):E349. doi: 10.9778/cmajo.20200239. Print 2021 Apr-Jun. CMAJ Open. 2021. PMID: 33849984 Free PMC article.
-
Risk of Adverse Neonatal Outcomes After Combined Prenatal Cannabis and Nicotine Exposure.JAMA Netw Open. 2024 May 1;7(5):e2410151. doi: 10.1001/jamanetworkopen.2024.10151. JAMA Netw Open. 2024. PMID: 38713462 Free PMC article.
-
Birth Outcomes of Neonates Exposed to Marijuana in Utero: A Systematic Review and Meta-analysis.JAMA Netw Open. 2022 Jan 4;5(1):e2145653. doi: 10.1001/jamanetworkopen.2021.45653. JAMA Netw Open. 2022. PMID: 35084479 Free PMC article.
-
Omega-3 fatty acid addition during pregnancy.Cochrane Database Syst Rev. 2018 Nov 15;11(11):CD003402. doi: 10.1002/14651858.CD003402.pub3. Cochrane Database Syst Rev. 2018. PMID: 30480773 Free PMC article.
Cited by
-
Impact of Acute and Chronic Cannabis Use on Stress Response Regulation: Challenging the Belief That Cannabis Is an Effective Method for Coping.Front Psychol. 2021 Jul 1;12:687106. doi: 10.3389/fpsyg.2021.687106. eCollection 2021. Front Psychol. 2021. PMID: 34276511 Free PMC article. Review.
-
Prevalence of Prenatal Opioid Exposure in Ontario, Canada, 2014-2019.JAMA Netw Open. 2021 Feb 1;4(2):e2037388. doi: 10.1001/jamanetworkopen.2020.37388. JAMA Netw Open. 2021. PMID: 33595660 Free PMC article.
-
Use of prescription opioids and other psychotropic drugs during pregnancy and their impact on the mother and developing child: protocol for a cohort study using linked administrative data from Manitoba and British Columbia, Canada.BMJ Open. 2025 May 2;15(5):e097657. doi: 10.1136/bmjopen-2024-097657. BMJ Open. 2025. PMID: 40316364 Free PMC article.
-
Prenatal Opioid Use Disorder and the Risk of Congenital Anomalies in Offspring: A Population-Based Study.Birth Defects Res. 2025 Feb;117(2):e2456. doi: 10.1002/bdr2.2456. Birth Defects Res. 2025. PMID: 39976348 Free PMC article.
-
"They're not doing enough.": women's experiences with opioids and naloxone in Toronto.Subst Abuse Treat Prev Policy. 2021 Mar 20;16(1):26. doi: 10.1186/s13011-021-00360-3. Subst Abuse Treat Prev Policy. 2021. PMID: 33743756 Free PMC article.
References
-
- Canadian Institute for Health Information . Opioid-Related Harms in Canada. CIHI; September 2017. Accessed March 19, 2020. https://secure.cihi.ca/free_products/opioid-harms-chart-book-en.pdf
-
- Special Advisory Committee on the Epidemic of Opioid Overdoses . National Report: Apparent Opioid-Related Deaths in Canada. Public Health Agency of Canada. Published March 2018. Updated March 17, 2020. Accessed March 19, 2020. https://www.canada.ca/en/public-health/services/publications/healthy-liv...
-
- Mattson CL, Schieber L, Scholl L, et al. . National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Annual surveillance report of drug-related risks and outcomes: United States, 2017. Published August 31, 2017. Accessed June 25, 2020. https://www.cdc.gov/drugoverdose/pdf/pubs/2017-cdc-drug-surveillance-rep...
-
- Salihu HM, Salemi JL, Aggarwal A, et al. . Opioid drug use and acute cardiac events among pregnant women in the United States. Am J Med. 2018;131(1):64-71.e1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
