

Implantation of a new active bone conduction hearing device with optimized geometry
- PMID: 32725263
- PMCID: PMC7403170
- DOI: 10.1007/s00106-020-00877-2
Implantation of a new active bone conduction hearing device with optimized geometry
Abstract
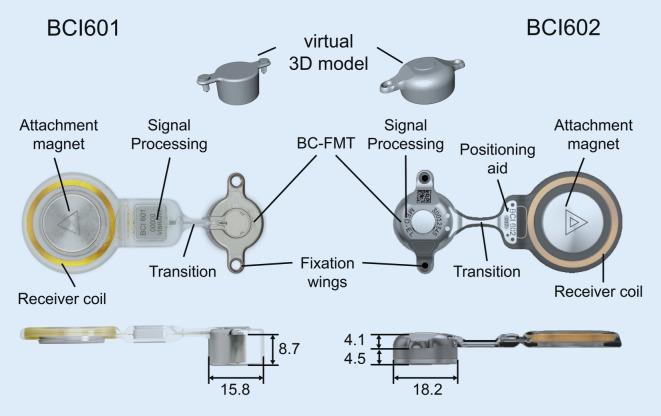
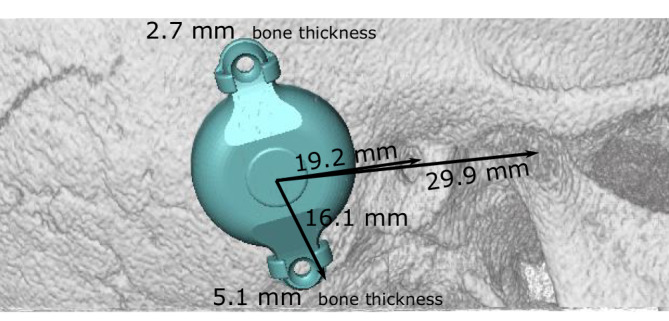
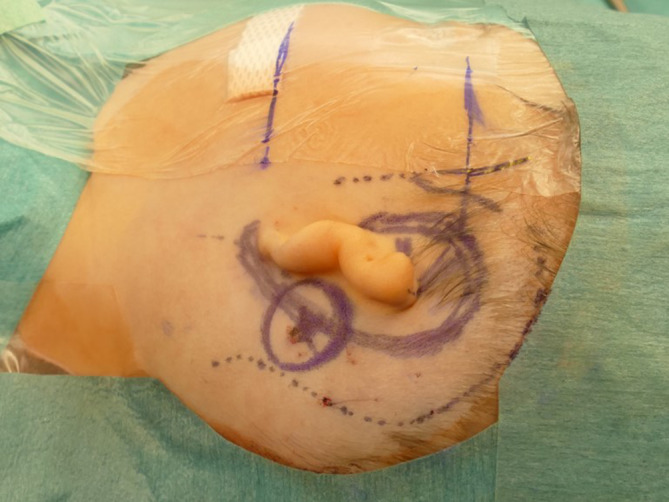
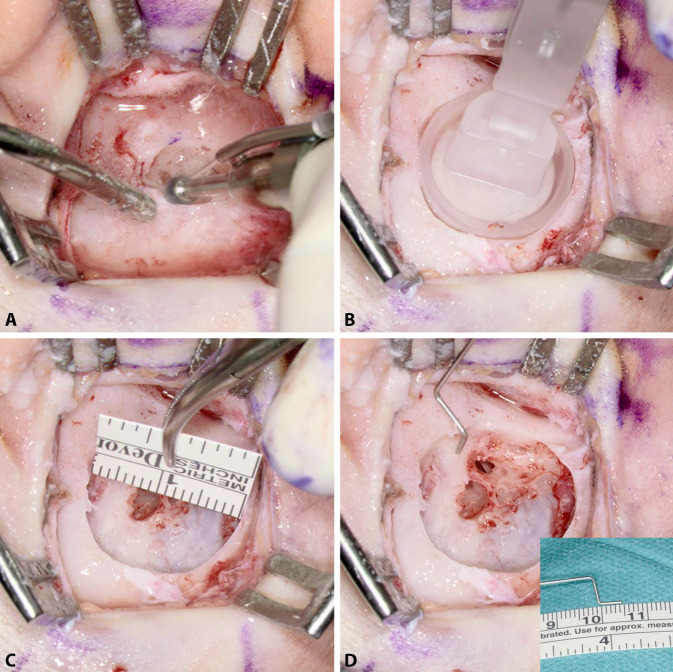
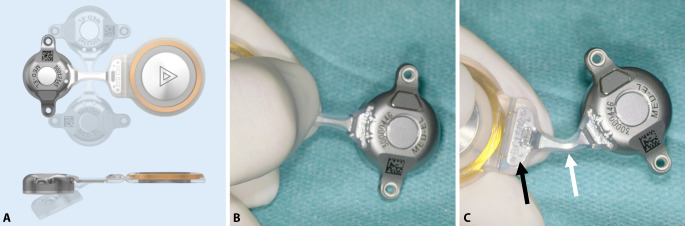
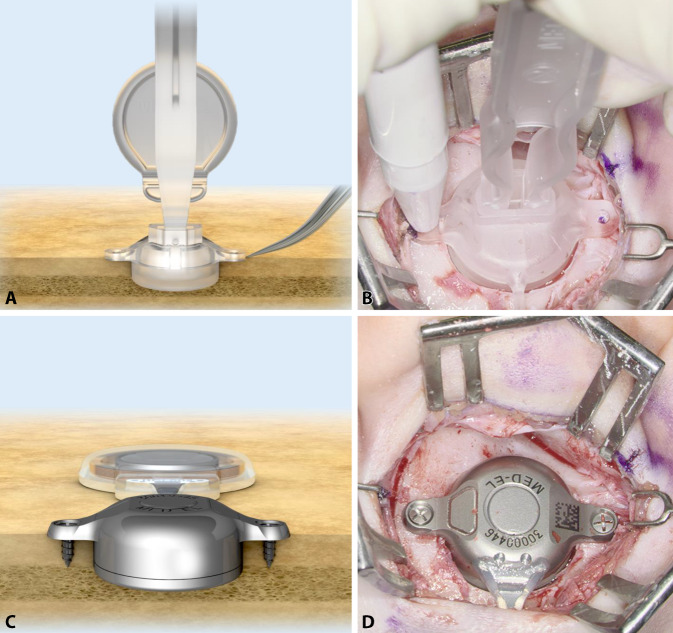
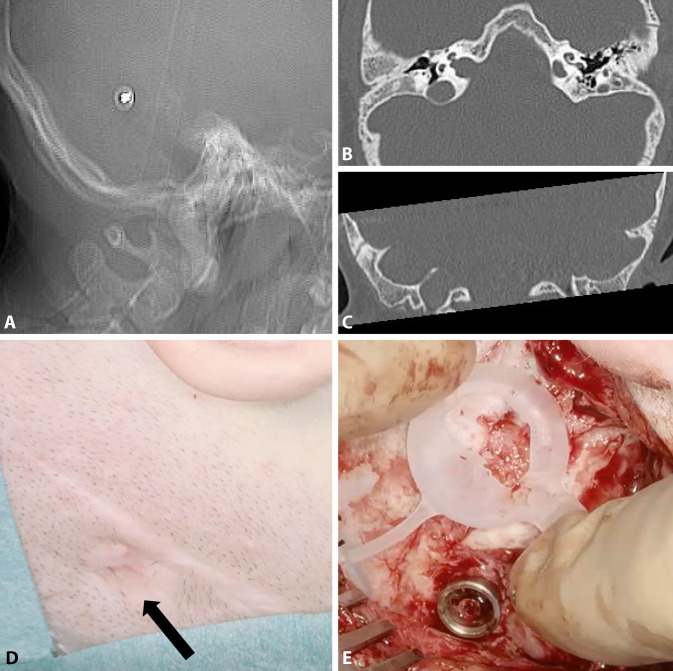
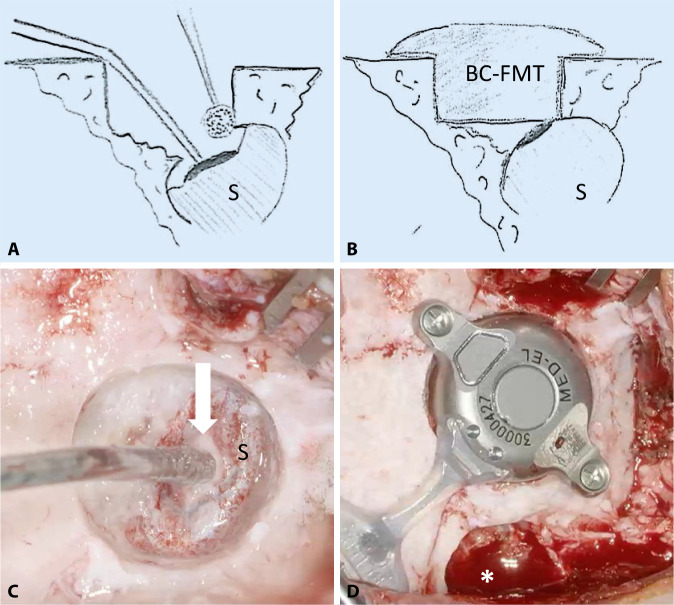
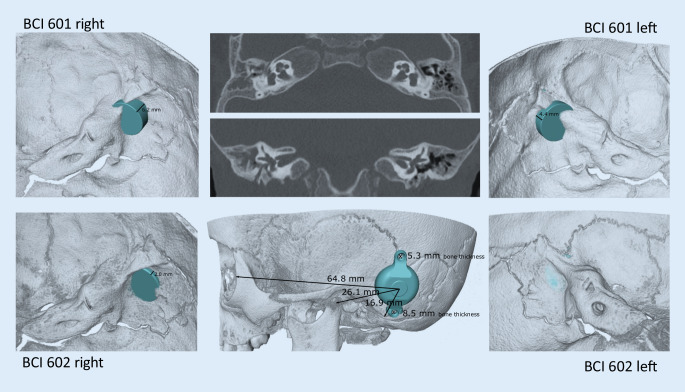
Here, we describe the surgical technique for implanting a new, active, transcutaneous bone conduction hearing aid. The implant technology is based on a system that has been in use reliably since 2012. The geometry of the new implant has been adapted based on experience with previously introduced implants. The surgery was feasible, standardized, and safe. Due to the optimized geometric design that improved the bone fit, it is not necessary to use specialized, detailed preoperative planning, except in challenging anatomical conditions; e.g., in young children, malformations, poor pneumatization, or after a canal wall down mastoidectomy.
Keywords: Hearing aids; Hearing loss, conductive; Hearing loss, mixed, conductive-sensorineural; Otologic surgical procedures; Patients.
Conflict of interest statement
S.K. Plontke: Audio Cure Pharma GmbH, Berlin (consultancy); Oticon Medical, Denmark; Cochlear Ltd., Australia; Federal Ministry of Research and Education (Research Projects); BV-HNOe.V.; MerckSerono; Infectopharm; Dr.Willmar Schwabe GmbH& Co. KG, Deutschland (honrary for lectures and travel support for lectures). T. Rahne: Oticon Medical,Denmark; Cochlear Ltd., Australia (Research Projects). S.K. Plontke, G. Götze, C. Wenzel, T. Rahne, and R.Mlynski: MED-EL, Austria, and MED-EL Germany (Research Projects); MED-EL Austria and MED-EL Germany (travel support for lectures).
Figures

References
-
- Anonymous MED-EL Medical Electronics. Bonebridge (BCI 602) Surgical Guide V 2.0 (2019). In: MED-EL, Innsbruck, Austria
-
- Arnold H, Schulze M, Wolpert S, et al. Positioning a novel transcutaneous bone conduction hearing implant: a systematic anatomical and radiological study to standardize the retrosigmoid approach, correlating navigation-guided, and landmark-based surgery. Otol Neurotol. 2018;39:458–466. - PubMed
-
- Beutner D, Delb W, Frenzel H, et al. Guideline “Implantable hearing aids”-short version : German S2k guideline of the Working Group of German-speaking Audiologists, Neurootologists and Otologists (ADANO), of the German Society of Oto-Rhino-Laryngology, Head and Neck Surgery (DGHNO) in collaboration with the German Society of Audiology (DGA), the German Society of Phoniatrics and Pediatric Audiology (DGPP), and patient representatives. HNO. 2018;66:654–659. doi: 10.1007/s00106-018-0531-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
