

Point-of-care Lung Ultrasound Is More Sensitive than Chest Radiograph for Evaluation of COVID-19
- PMID: 32726240
- PMCID: PMC7390587
- DOI: 10.5811/westjem.2020.5.47743
Point-of-care Lung Ultrasound Is More Sensitive than Chest Radiograph for Evaluation of COVID-19
Abstract
Introduction: Current recommendations for diagnostic imaging for moderately to severely ill patients with suspected coronavirus disease 2019 (COVID-19) include chest radiograph (CXR). Our primary objective was to determine whether lung ultrasound (LUS) B-lines, when excluding patients with alternative etiologies for B-lines, are more sensitive for the associated diagnosis of COVID-19 than CXR.
Methods: This was a retrospective cohort study of all patients who presented to a single, academic emergency department in the United States between March 20 and April 6, 2020, and received LUS, CXR, and viral testing for COVID-19 as part of their diagnostic evaluation. The primary objective was to estimate the test characteristics of both LUS B-lines and CXR for the associated diagnosis of COVID-19. Our secondary objective was to evaluate the proportion of patients with COVID-19 that have secondary LUS findings of pleural abnormalities and subpleural consolidations.
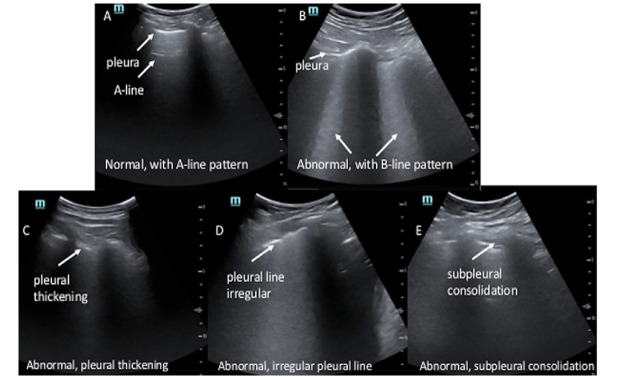
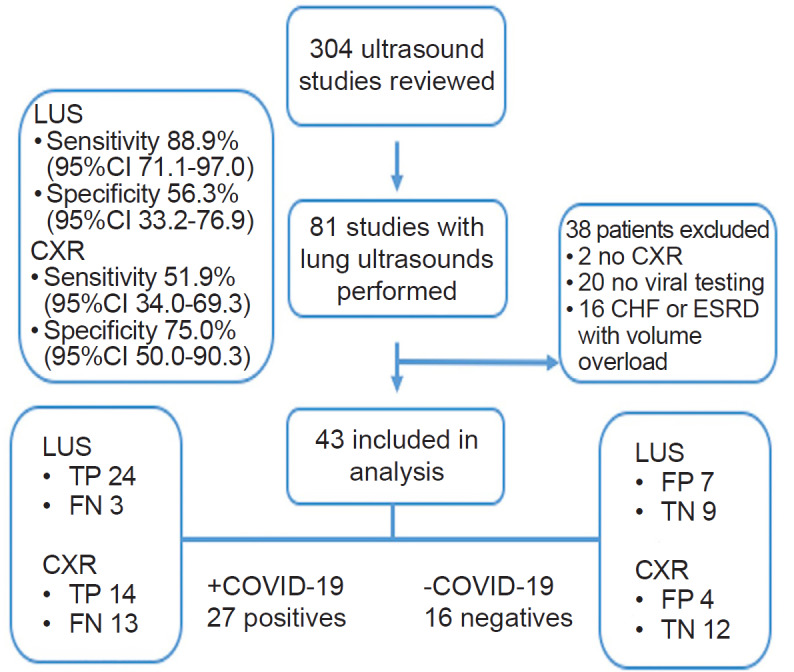
Results: We identified 43 patients who underwent both LUS and CXR and were tested for COVID-19. Of these, 27/43 (63%) tested positive. LUS was more sensitive (88.9%, 95% confidence interval (CI), 71.1-97.0) for the associated diagnosis of COVID-19 than CXR (51.9%, 95% CI, 34.0-69.3; p = 0.013). LUS and CXR specificity were 56.3% (95% CI, 33.2-76.9) and 75.0% (95% CI, 50.0-90.3), respectively (p = 0.453). Secondary LUS findings of patients with COVID-19 demonstrated 21/27 (77.8%) had pleural abnormalities and 10/27 (37%) had subpleural consolidations.
Conclusion: Among patients who underwent LUS and CXR, LUS was found to have a higher sensitivity than CXR for the evaluation of COVID-19. This data could have important implications as an aid in the diagnostic evaluation of COVID-19, particularly where viral testing is not available or restricted. If generalizable, future directions would include defining how to incorporate LUS into clinical management and its role in screening lower-risk populations.
Conflict of interest statement
Figures
References
-
- Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307(23):2526–33. - PubMed
-
- American College of Radiology. [Accessed April 7, 2020];ACR Recommendations for the Use of Chest Radiography and Computed Tomography (CT) for Suspected COVID-19 Infection. 2020 Available at: https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recom....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous