

Improved patient satisfaction and diagnostic accuracy in skin diseases with a Visual Clinical Decision Support System-A feasibility study with general practitioners
- PMID: 32726308
- PMCID: PMC7390264
- DOI: 10.1371/journal.pone.0235410
Improved patient satisfaction and diagnostic accuracy in skin diseases with a Visual Clinical Decision Support System-A feasibility study with general practitioners
Abstract
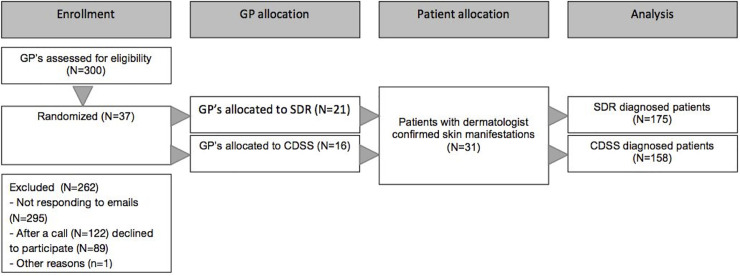
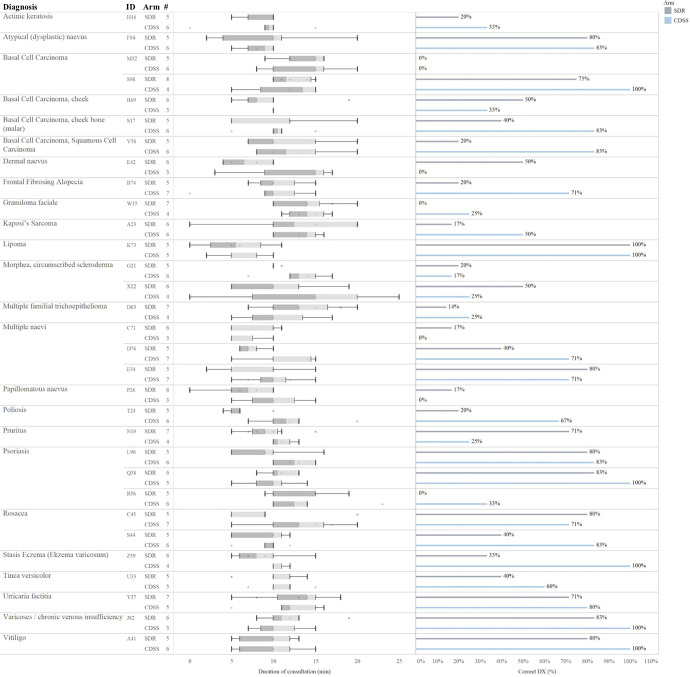
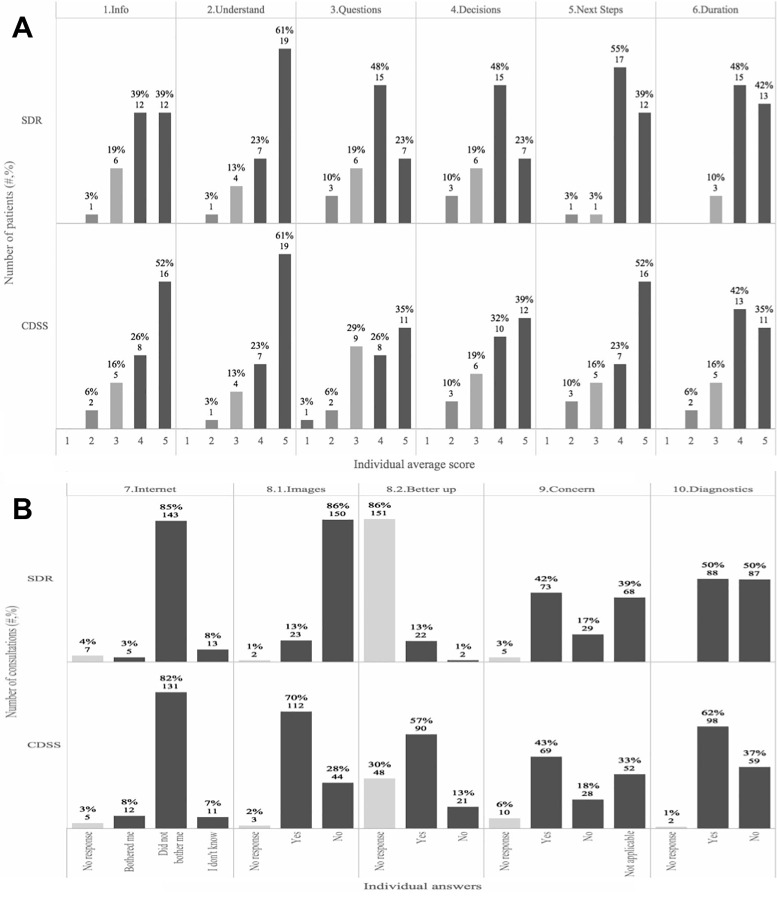
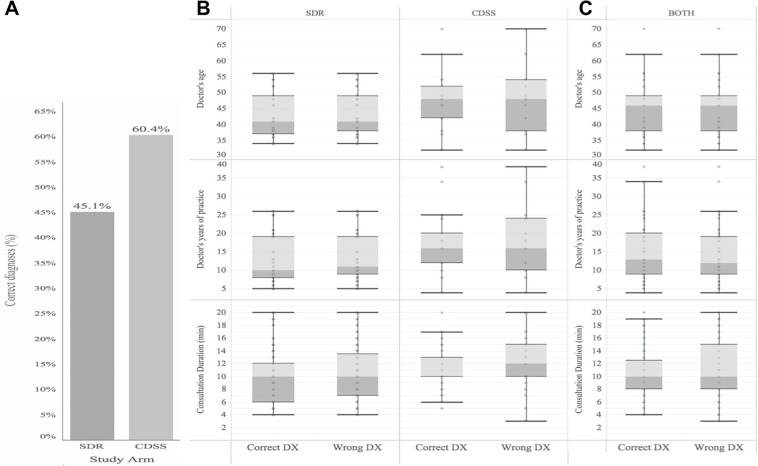
Patient satisfaction is an important indicator of health care quality, and it remains an important goal for optimal treatment outcomes to reduce the level of misdiagnoses and inappropriate or absent therapeutic actions. Digital support tools for differential diagnosis to assist clinicians in reaching the correct diagnosis may be helpful, but how the use of these affect patients is not clear. The primary objective of this feasibility study was to investigate patient experience and satisfaction in a primary care setting where general practitioners (GPs) used a visual clinical decision support system (CDSS) compared with standard consultations. Secondary objectives were diagnostic accuracy and length of consultation. Thirty-one patients with a dermatologist-confirmed skin diagnosis were allocated to consult GPs that had been randomized to conduct either standard consultations (SDR, n = 21) or CDSS (n = 16) on two separate study days one week apart. All patients were diagnosed independently by multiple GPs (n = 3-8) in both the SDR and CDSS study arms. Using the CDSS, more patients felt involved in the decision making (P = 0.05). In addition, more patients were exposed to images during the consultations (P = 6.8e-27), and 83% of those that were shown images replied they felt better supported in the consultation. The use of CDSS significantly improved the diagnostic accuracy (34%, P = 0.007), and did not increase the duration of the consultation (median 10 minutes in both arms). This study shows for the first time that compared with standard GP consultations, CDSS assist the GP on skin related diagnoses and improve patient satisfaction and diagnostic accuracy without impacting the duration of the consultations. This is likely to increase correct treatment choices, patient adherence, and overall result in better healthcare outcomes.
Conflict of interest statement
EB, KC, HB, and SF declare no competing financial interests. AMS, ADA, and JRZ are employees of LEO Innovation Lab, this does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
