

Impact of initial dialysis modality on the survival of patients with ESRD in eastern China: a propensity-matched study
- PMID: 32727426
- PMCID: PMC7389640
- DOI: 10.1186/s12882-020-01909-3
Impact of initial dialysis modality on the survival of patients with ESRD in eastern China: a propensity-matched study
Abstract
Background: There are conflicting research results about the survival differences between hemodialysis(HD) and peritoneal dialysis (PD). The present study estimated the survival and the relative mortality hazard for incident HD and PD patients with end stage renal disease (ESRD) in eastern China.
Methods: This study examined a cohort of patients with ESRD who initiated dialysis therapy in Zhejiang province between Jan of 2010 and Dec of 2014, followed up until the end of 2015. PD patients were matched in a 1:1 fashion with HD patients, and Kaplan-Meier analysis was used to explore the survival of them. The Cox proportional hazard regression model was applied to identify the factors that predict survival by treatment modality. Subgroup analyses were conducted by stratifying patients according to gender, age, causes of ESRD and comorbidities.
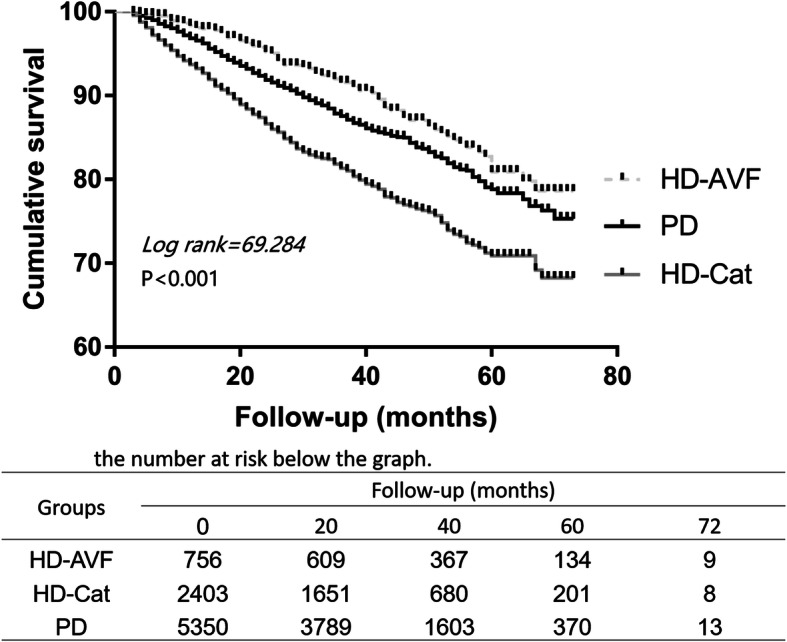
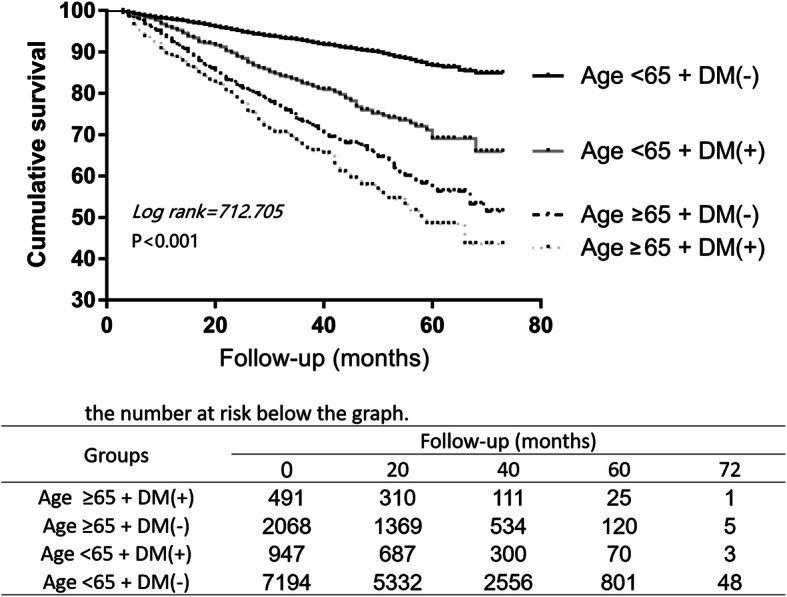
Results: Among a total of 22,379 enrolled patients (17,029 HD patients and 5350 PD patients), 5350 matched pairs were identified, and followed for a median of 29 months (3 ~ 72 months). Kaplan-Meier survival curve revealed that overall mortality rate was significantly higher in HD patients than in PD patients (log-rank test, P < 0.001), after adjusting by gender, age, primary causes of ESRD and comorbidities. HD was consistently associated with an increased risk for morality compared with PD in the matched cohort (adjusted hazard ratio (AHR): 1.140, 95%CI: 1.023 ~ 1.271). In subgroup analyses, male, younger patients, or nondiabetic patients aged less than 65 years after adjustment of covariates, initiating with PD was associated with a significantly lower mortality compared with HD. In the multivariate Cox proportional risks model, age, diabetic nephropathy (DN), other/unknown causes of ESRD, and patients with a history of cardiovascular disease or cancer showed statistical significance in explaining survival of incident ESRD patients.
Conclusions: ESRD patients who initiated dialysis with PD yielded superior survival rates compared to HD. Increased use of PD as initial dialysis modality in ESRD patients could be encouraged in Chinese population.
Keywords: End stage renal disease (ESRD); Hemodialysis; Mortality; Peritoneal dialysis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Puddu PE, Piras P, Menotti A. Competing risks and lifetime coronary heart disease incidence during 50years of follow-up. Int J Cardiol. 2016;219:79–83. - PubMed
-
- Kramer A, Pippias M, Noordzij M, Stel VS, Andrusev AM, Aparicio-Madre MI, Arribas Monzon FE, Asberg A, Barbullushi M, Beltran P, et al. The European renal association - European Dialysis and transplant association (ERA-EDTA) registry annual report 2016: a summary. Clin Kidney J. 2019;12(5):702–720. - PMC - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
