

In-hospital mortality and failure to rescue following hepatobiliary surgery in Germany - a nationwide analysis
- PMID: 32727457
- PMCID: PMC7388497
- DOI: 10.1186/s12893-020-00817-5
In-hospital mortality and failure to rescue following hepatobiliary surgery in Germany - a nationwide analysis
Abstract
Background: Recent observational studies on volume-outcome associations in hepatobiliary surgery were not designed to account for the varying extent of hepatobiliary resections and the consequential risk of perioperative morbidity and mortality. Therefore, this study aimed to determine the risk-adjusted in-hospital mortality for minor and major hepatobiliary resections at the national level in Germany and to examine the effect of hospital volume on in-hospital mortality, and failure to rescue.
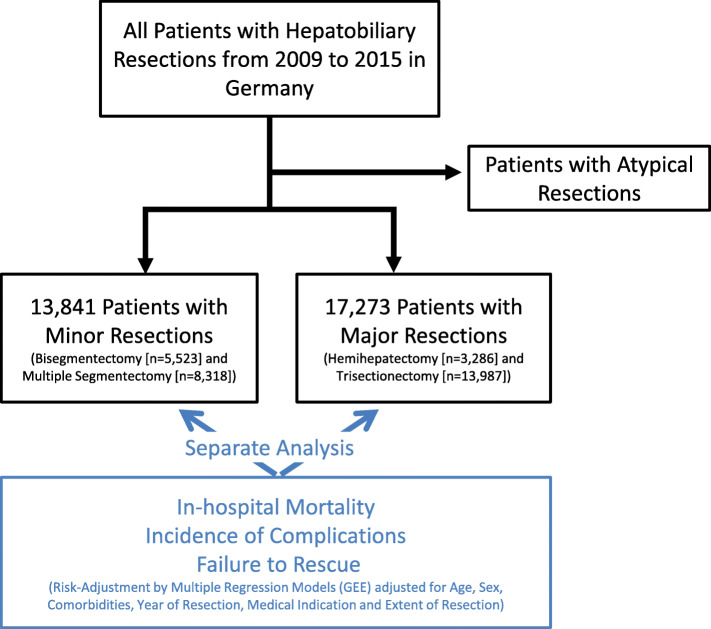
Methods: All inpatient cases of hepatobiliary surgery (n = 31,114) in Germany from 2009 to 2015 were studied using national hospital discharge data. After ranking hospitals according to increasing hospital volumes, five volume categories were established based on all hepatobiliary resections. The association between hospital volume and in-hospital mortality following minor and major hepatobiliary resections was evaluated by multivariable regression methods.
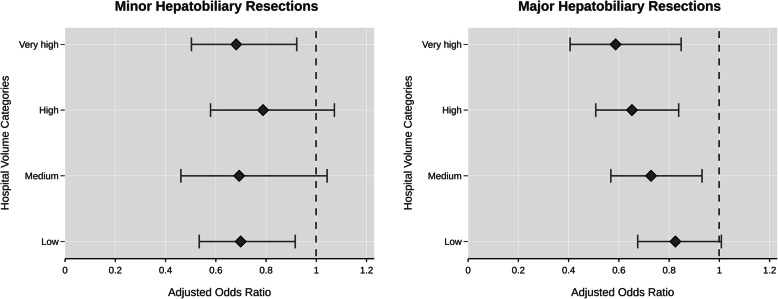
Results: Minor hepatobiliary resections were associated with an overall mortality rate of 3.9% and showed no significant volume-outcome associations. In contrast, overall mortality rate of major hepatobiliary resections was 10.3%. In this cohort, risk-adjusted in-hospital mortality following major resections varied widely across hospital volume categories, from 11.4% (95% CI 10.4-12.5) in very low volume hospitals to 7.4% (95% CI 6.6-8.2) in very high volume hospitals (risk-adjusted OR 0.59, 95% CI 0.41-0.54). Moreover, rates of failure to rescue decreased from 29.38% (95% CI 26.7-32.2) in very low volume hospitals to 21.38% (95% CI 19.2-23.8) in very high volume hospitals.
Conclusions: In Germany, patients who are undergoing major hepatobiliary resections have improved outcomes, if they are admitted to higher volume hospitals. However, such associations are not evident following minor hepatobiliary resections. Following major hepatobiliary resections, 70-80% of the excess mortality in very low volume hospitals was estimated to be attributable to failure to rescue.
Conflict of interest statement
None.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
