

Impact of lockdown on COVID-19 epidemic in Île-de-France and possible exit strategies
- PMID: 32727547
- PMCID: PMC7391016
- DOI: 10.1186/s12916-020-01698-4
Impact of lockdown on COVID-19 epidemic in Île-de-France and possible exit strategies
Abstract
Background: More than half of the global population is under strict forms of social distancing. Estimating the expected impact of lockdown and exit strategies is critical to inform decision makers on the management of the COVID-19 health crisis.
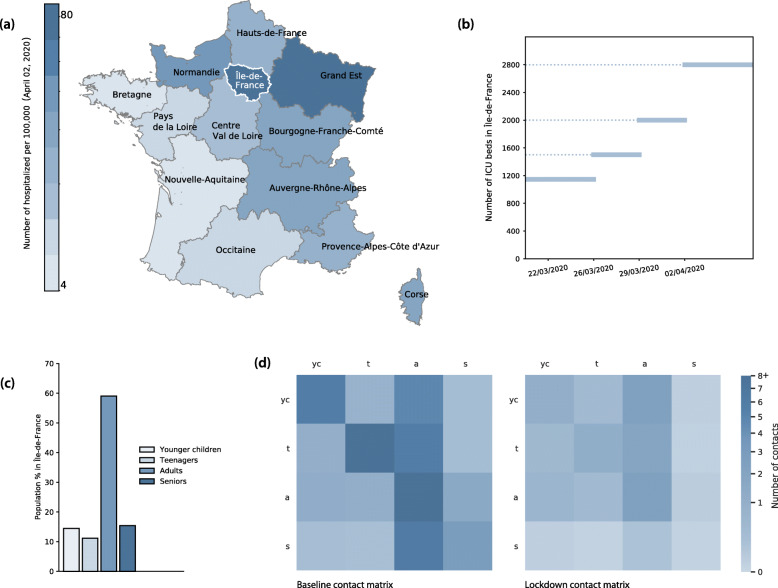
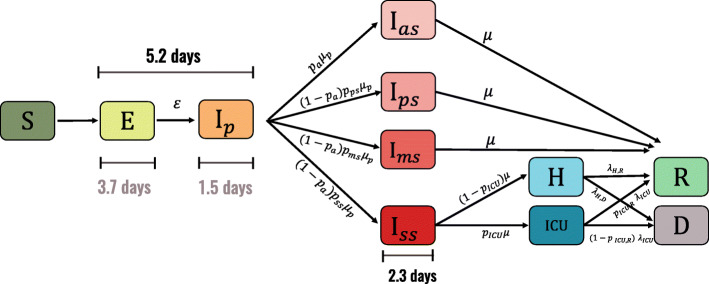
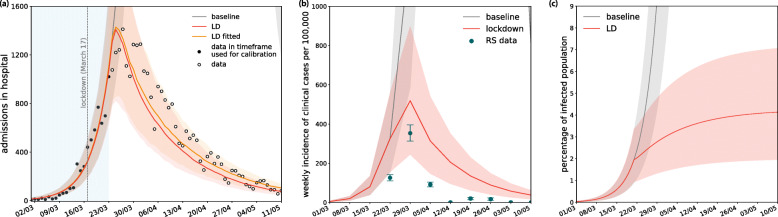
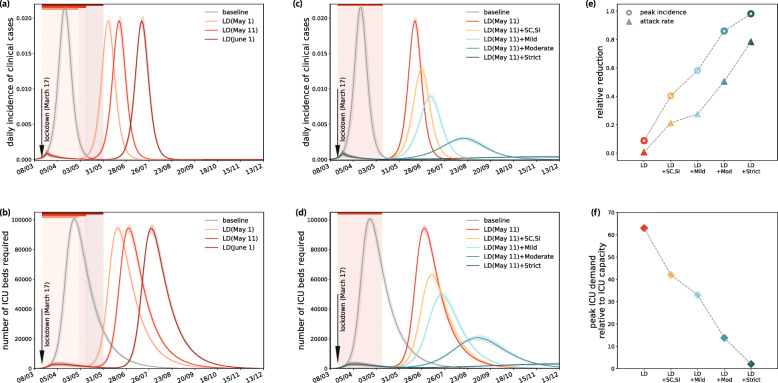
Methods: We use a stochastic age-structured transmission model integrating data on age profile and social contacts in Île-de-France to (i) assess the epidemic in the region, (ii) evaluate the impact of lockdown, and (iii) propose possible exit strategies and estimate their effectiveness. The model is calibrated to hospital admission data before lockdown. Interventions are modeled by reconstructing the associated changes in the contact matrices and informed by mobility reductions during lockdown evaluated from mobile phone data. Different types and durations of social distancing are simulated, including progressive and targeted strategies, with large-scale testing.
Results: We estimate the reproductive number at 3.18 [3.09, 3.24] (95% confidence interval) prior to lockdown and at 0.68 [0.66, 0.69] during lockdown, thanks to an 81% reduction of the average number of contacts. Model predictions capture the disease dynamics during lockdown, showing the epidemic curve reaching ICU system capacity, largely strengthened during the emergency, and slowly decreasing. Results suggest that physical contacts outside households were largely avoided during lockdown. Lifting the lockdown with no exit strategy would lead to a second wave overwhelming the healthcare system, if conditions return to normal. Extensive case finding and isolation are required for social distancing strategies to gradually relax lockdown constraints.
Conclusions: As France experiences the first wave of COVID-19 pandemic in lockdown, intensive forms of social distancing are required in the upcoming months due to the currently low population immunity. Extensive case finding and isolation would allow the partial release of the socio-economic pressure caused by extreme measures, while avoiding healthcare demand exceeding capacity. Response planning needs to urgently prioritize the logistics and capacity for these interventions.
Keywords: COVID-19; Exit strategies; Lockdown; Mathematical modeling; Non-pharmaceutical interventions; Reproductive number; Social distancing.
Conflict of interest statement
We declare no competing interests.
Figures



References
-
- Coronavirus: près de la moitié du monde en confinement, l’épidémie s’étend. AFP.com. https://www.afp.com/fr/infos/334/coronavirus-pres-de-la-moitie-du-monde-.... Accessed 28 Mar 2020.
-
- Epicentre. COVID-19 Epi Dashboard. https://reports.msf.net/public/covid19/. Accessed 5 Apr 2020.
-
- Info Coronavirus COVID-19 - Stratégie de déconfinement. Gouvernement.fr. https://www.gouvernement.fr/info-coronavirus/strategie-de-deconfinement. Accessed 4 May 2020.
-
- WHO. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mis.... Accessed 18 Mar 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
