

Global prevalence and distribution of vancomycin resistant, vancomycin intermediate and heterogeneously vancomycin intermediate Staphylococcus aureus clinical isolates: a systematic review and meta-analysis
- PMID: 32728110
- PMCID: PMC7391782
- DOI: 10.1038/s41598-020-69058-z
Global prevalence and distribution of vancomycin resistant, vancomycin intermediate and heterogeneously vancomycin intermediate Staphylococcus aureus clinical isolates: a systematic review and meta-analysis
Abstract
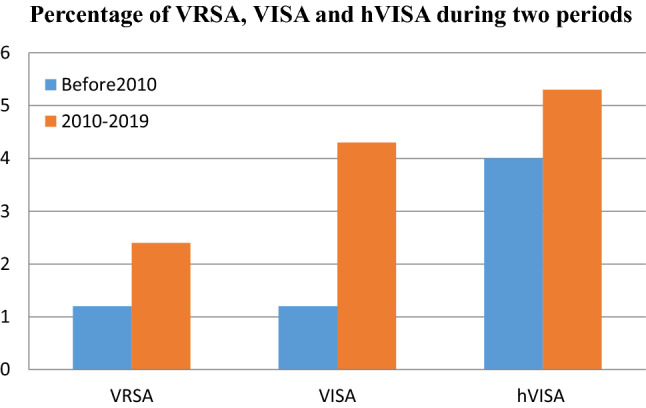
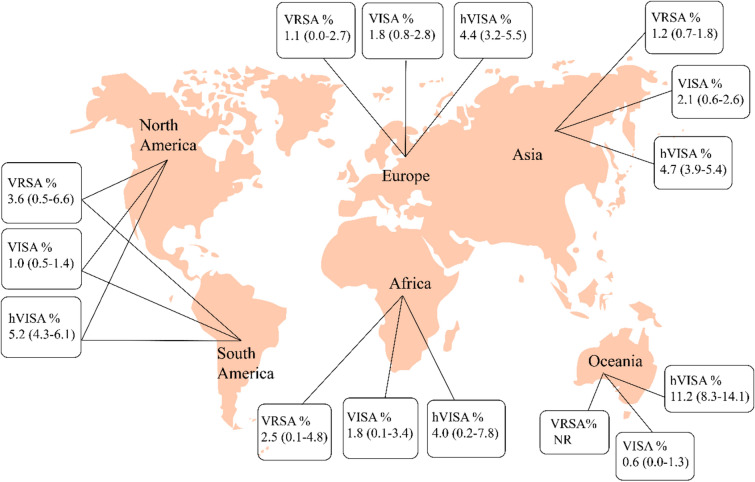
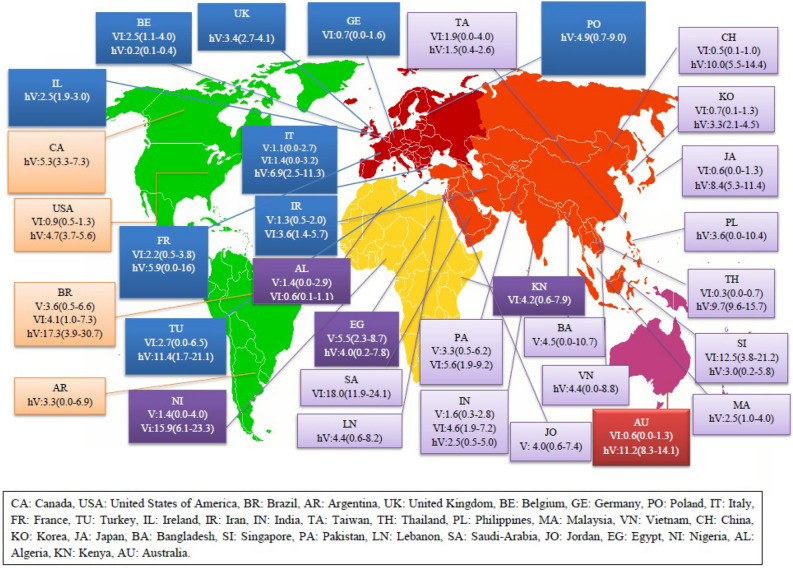
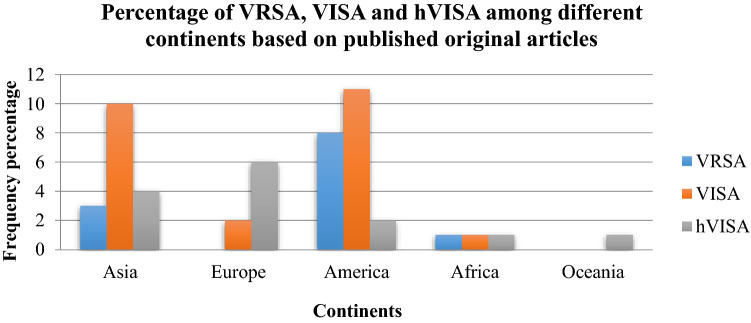
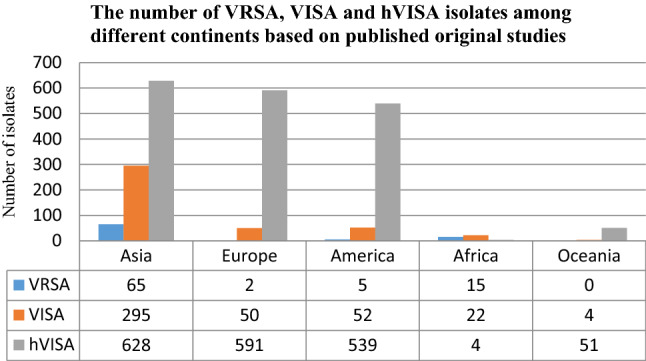
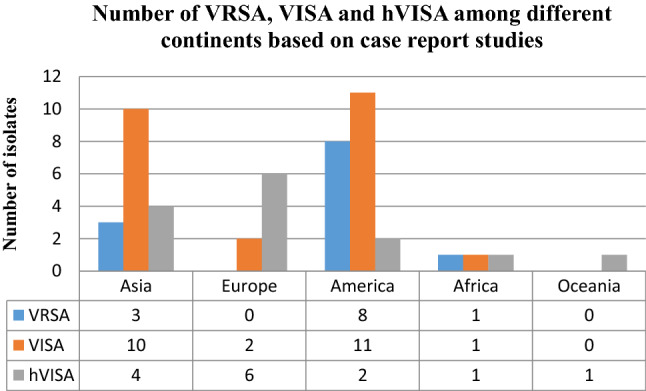
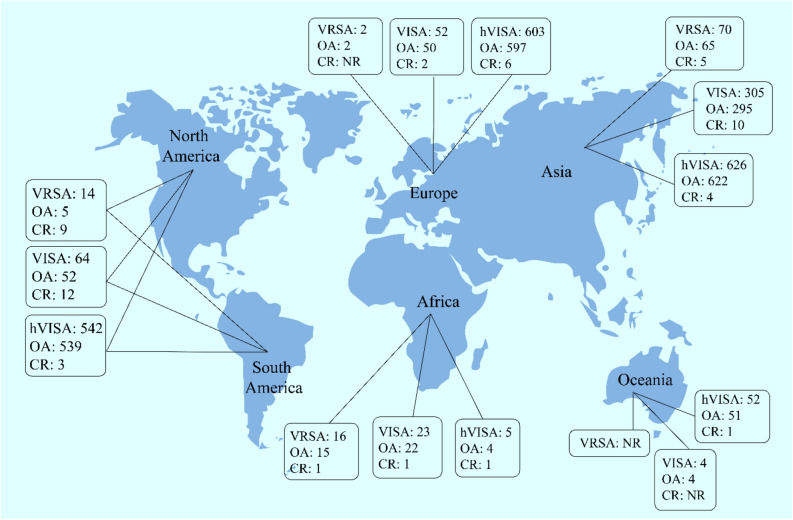
Vancomycin-resistant Staphylococcus aureus (VRSA), Vancomycin-intermediate S. aureus (VISA) and heterogeneous VISA (hVISA) are subject to vancomycin treatment failure. The aim of the present study was to determine their precise prevalence and investigate prevalence variability depending on different years and locations. Several international databases including Medline (PubMed), Embase and Web of Sciences were searched (data from 1997 to 2019) to identify studies that addressed the prevalence of VRSA, VISA and hVISA among human clinical isolates around the world. Subgroup analyses and meta-regression were conducted to indicate potential source of variation. Publication bias was assessed using Egger's test. Statistical analyses were conducted using STATA software (version 14.0). Data analysis showed that VRSA, VISA and hVISA isolates were reported in 23, 50 and 82 studies, with an overall prevalence of 1.5% among 5855 S. aureus isolates, 1.7% among 22,277 strains and 4.6% among 47,721 strains, respectively. The overall prevalence of VRSA, VISA, and hVISA before 2010 was 1.2%, 1.2%, and 4%, respectively, while their prevalence after this year has reached 2.4%, 4.3%, and 5.3%. The results of this study showed that the frequency of VRSA, VISA and hVISA after 2010 represent a 2.0, 3.6 and 1.3-fold increase over prior years. In a subgroup analysis of different strain origins, the highest frequency of VRSA (3.6%) and hVISA (5.2%) was encountered in the USA while VISA (2.1%) was more prevalent in Asia. Meta-regression analysis showed significant increasing of VISA prevalence in recent years (p value ≤ 0.05). Based on the results of case reports (which were not included in the calculations mentioned above), the numbers of VRSA, VISA and hVISA isolates were 12, 24 and 14, respectively, among different continents. Since the prevalence of VRSA, VISA and hVISA has been increasing in recent years (especially in the Asian and American continents), rigorous monitoring of vancomycin treatment, it's the therapeutic response and the definition of appropriate control guidelines depending on geographical regions is highly recommended and essential to prevent the further spread of vancomycin-resistant S. aureus.
Conflict of interest statement
Alex van Belkum is a bioMerieux employee. bioMerieux is a company that design, develops and sells diagnostics in the field on infectious diseases. The company had no direct influence on the design and execution of the present study. Rest of the authors declare to have no competing interest.
Figures

References
-
- Shanson D, Kensit J, Duke R. Outbreak of hospital infection with a strain of Staphylococcus aureus resistant to gentamicin and methicillin. The Lancet. 1976;308:1347–1348. - PubMed
-
- Haley RW, et al. The emergence of methicillin-resistant Staphylococcus aureus infections in United States hospitals: possible role of the house staff-patient transfer circuit. Ann. Internal Med. 1982;97:297–308. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
