

Efficacy of PD-1/PD-L1 blockade monotherapy in clinical trials
- PMID: 32728392
- PMCID: PMC7366397
- DOI: 10.1177/1758835920937612
Efficacy of PD-1/PD-L1 blockade monotherapy in clinical trials
Abstract
Background: Inhibitors targeting programmed cell death 1 (PD-1) and programmed death-ligand 1 (PD-L1) have unprecedented effects in cancer treatment. However, the objective response rates (ORRs), progression-free survival (PFS), and overall survival (OS) of PD-1/PD-L1 blockade monotherapy have not been systematically evaluated.
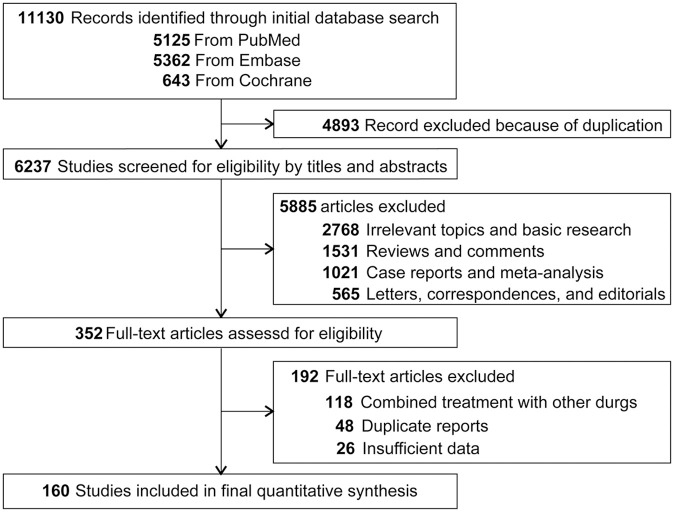
Methods: We searched Embase, PubMed, and Cochrane database from inception to July 2019 for prospective clinical trials on single-agent PD-1/PD-L1 antibodies (avelumab, atezolizumab, durvalumab, cemiplimab, pembrolizumab, and nivolumab) with information regarding ORR, PFS, and OS.
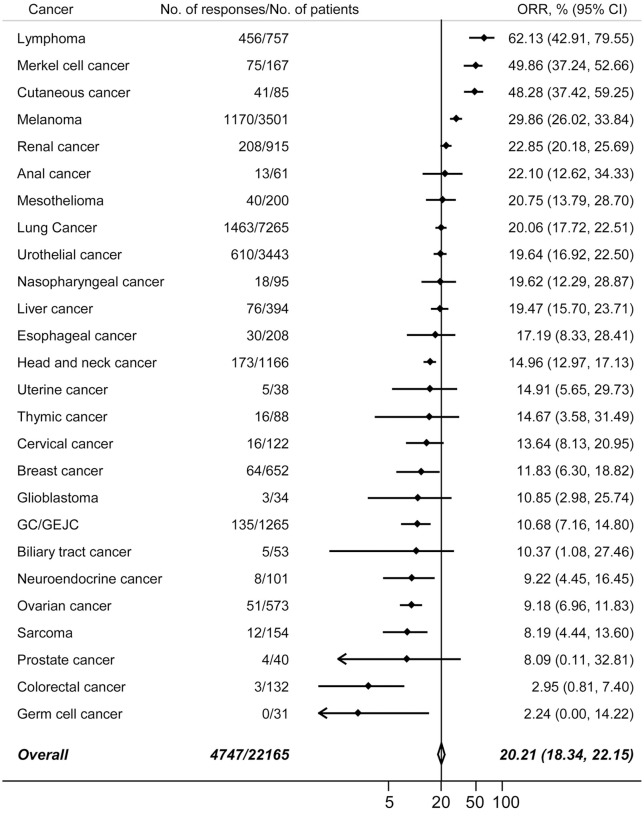
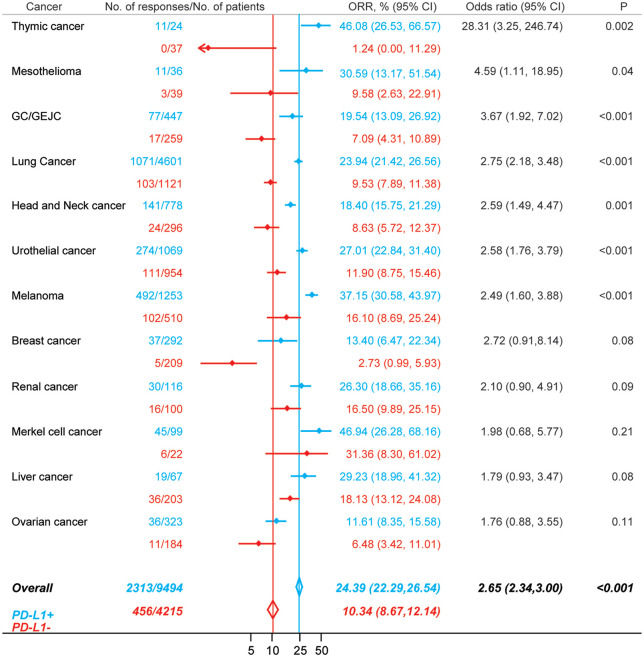
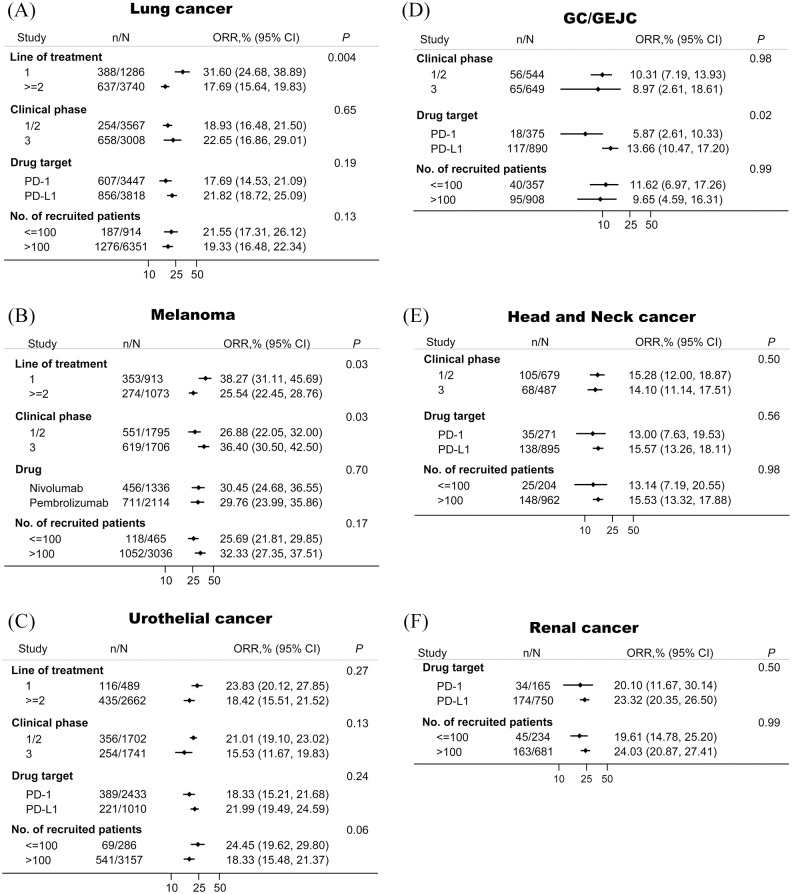
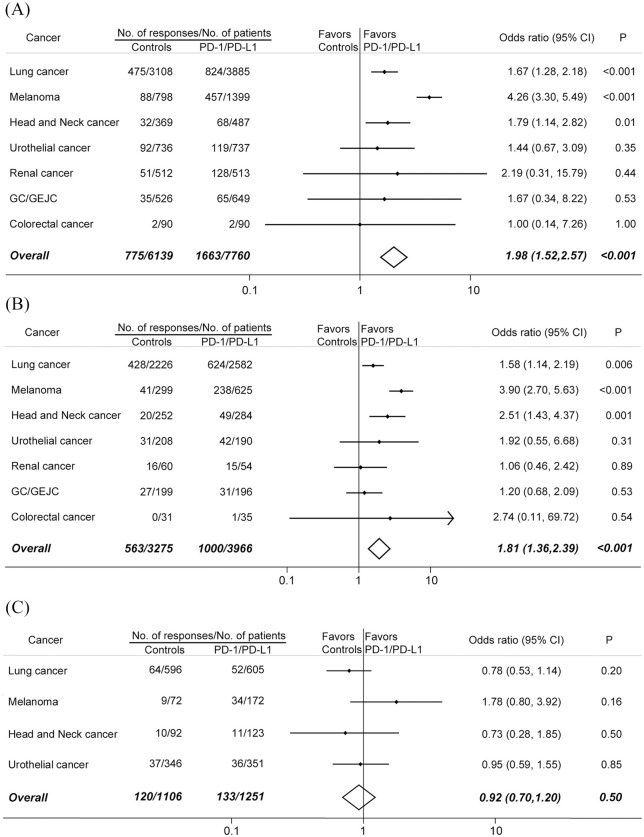
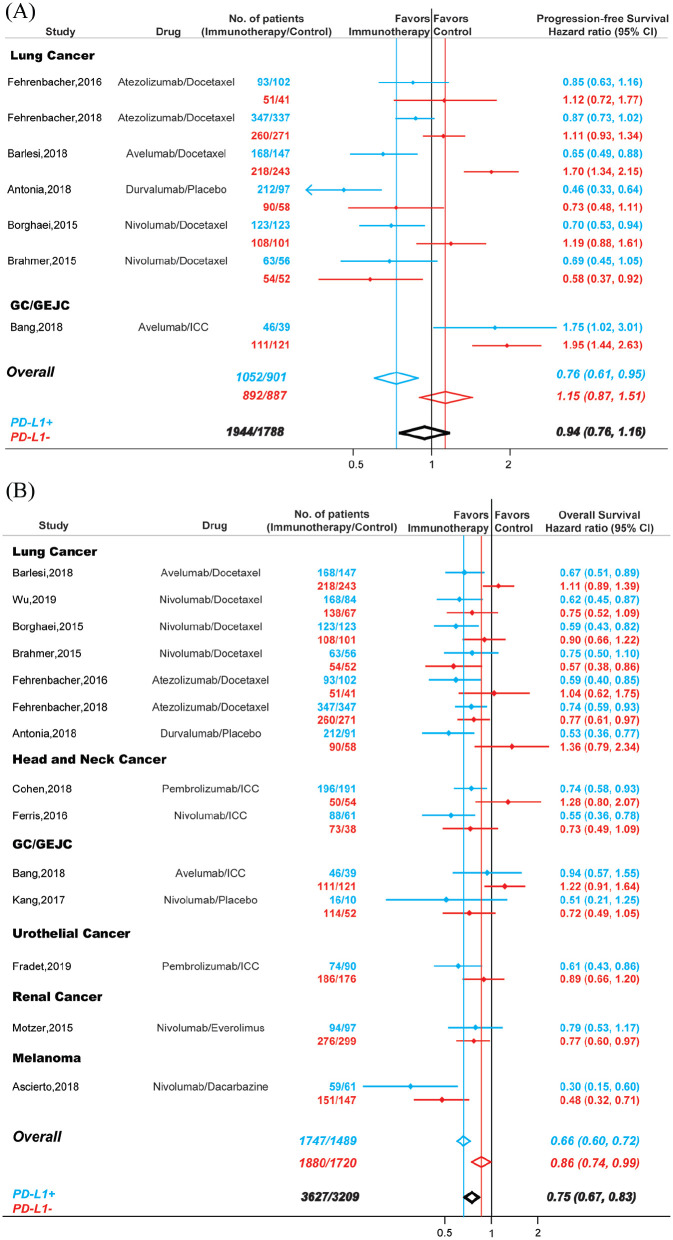
Results: Totally, 28,304 patients from 160 perspective trials were included. Overall, 4747 responses occurred in 22,165 patients treated with PD-1/PD-L1 monotherapy [ORR, 20.21%; 95% confidence interval (CI), 18.34-22.15%]. Compared with conventional therapy, PD-1/PD-L1 blockade immunotherapy was associated with more tumor responses (odds ratio, 1.98; 95% CI, 1.52-2.57) and better OS [hazard ratio (HR), 0.75; 95% CI, 0.67-0.83]. The ORRs varied significantly across cancer types and PD-L1 expression status. Line of treatment, clinical phase and drug target also impacted the response rates in some tumors. A total of 2313 of 9494 PD-L1 positive patients (ORR, 24.39%; 95% CI, 22.29-26.54%) and 456 of 4215 PD-L1 negative patients (ORR, 10.34%; 95% CI, 8.67-12.14%) achieved responses. For PD-L1 negative patients, the ORR (odds ratio, 0.92; 95% CI, 0.70-1.20) and PFS (HR, 1.15; 95% CI, 0.87-1.51) associated with immunotherapy and conventional treatment were similar. However, PD-1/PD-L1 blockade monotherapy decreased the risk of death in both PD-L1 positive (HR, 0.66; 95% CI, 0.60-0.72) and PD-L1 negative (HR, 0.86; 95% CI, 0.74-0.99) patients compared with conventional therapy.
Conclusion: The efficacies associated with PD-1/PD-L1 monotherapy vary significantly across cancer types and PD-L1 expression. This comprehensive summary of clinical benefit from immunotherapy in cancer patients provides an important guide for clinicians.
Keywords: PD-1; PD-L1; cancer; immunotherapy; tumor response.
© The Author(s), 2020.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996; 17: 1–12. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
