

Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS
- PMID: 32728965
- PMCID: PMC7387884
- DOI: 10.1007/s00134-020-06192-2
Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS
Erratum in
-
Correction to: Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS.Intensive Care Med. 2021 Jan;47(1):144-146. doi: 10.1007/s00134-020-06251-8. Intensive Care Med. 2021. PMID: 33263817 Free PMC article. No abstract available.
Abstract
Purpose: The main characteristics of mechanically ventilated ARDS patients affected with COVID-19, and the adherence to lung-protective ventilation strategies are not well known. We describe characteristics and outcomes of confirmed ARDS in COVID-19 patients managed with invasive mechanical ventilation (MV).
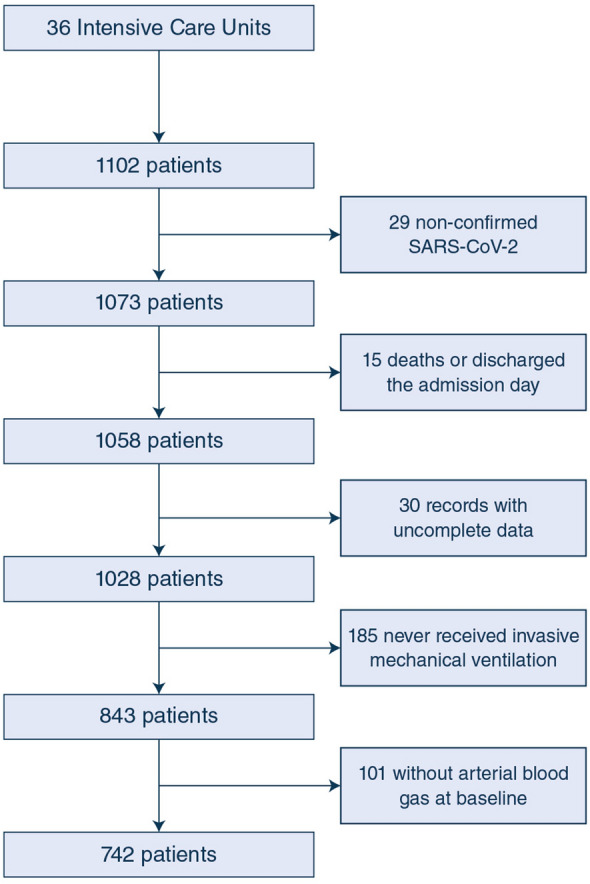
Methods: This is a multicenter, prospective, observational study in consecutive, mechanically ventilated patients with ARDS (as defined by the Berlin criteria) affected with with COVID-19 (confirmed SARS-CoV-2 infection in nasal or pharyngeal swab specimens), admitted to a network of 36 Spanish and Andorran intensive care units (ICUs) between March 12 and June 1, 2020. We examined the clinical features, ventilatory management, and clinical outcomes of COVID-19 ARDS patients, and compared some results with other relevant studies in non-COVID-19 ARDS patients.
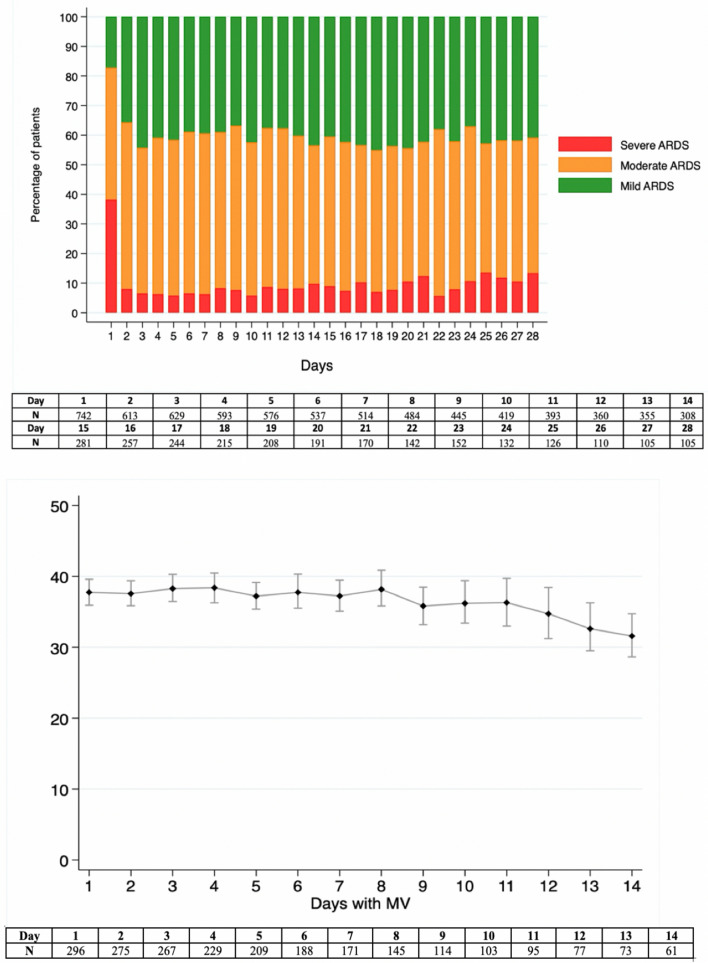
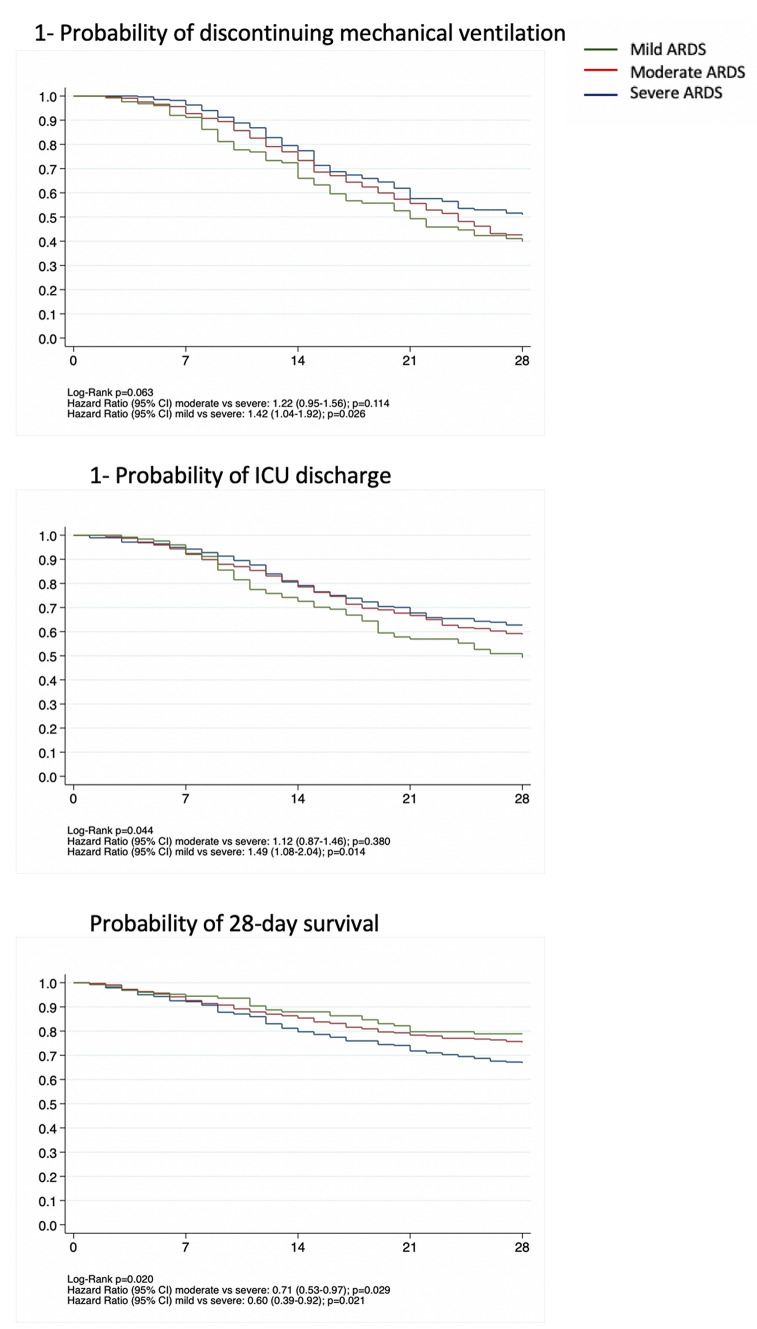
Results: A total of 742 patients were analysed with complete 28-day outcome data: 128 (17.1%) with mild, 331 (44.6%) with moderate, and 283 (38.1%) with severe ARDS. At baseline, defined as the first day on invasive MV, median (IQR) values were: tidal volume 6.9 (6.3-7.8) ml/kg predicted body weight, positive end-expiratory pressure 12 (11-14) cmH2O. Values of respiratory system compliance 35 (27-45) ml/cmH2O, plateau pressure 25 (22-29) cmH2O, and driving pressure 12 (10-16) cmH2O were similar to values from non-COVID-19 ARDS patients observed in other studies. Recruitment maneuvers, prone position and neuromuscular blocking agents were used in 79%, 76% and 72% of patients, respectively. The risk of 28-day mortality was lower in mild ARDS [hazard ratio (RR) 0.56 (95% CI 0.33-0.93), p = 0.026] and moderate ARDS [hazard ratio (RR) 0.69 (95% CI 0.47-0.97), p = 0.035] when compared to severe ARDS. The 28-day mortality was similar to other observational studies in non-COVID-19 ARDS patients.
Conclusions: In this large series, COVID-19 ARDS patients have features similar to other causes of ARDS, compliance with lung-protective ventilation was high, and the risk of 28-day mortality increased with the degree of ARDS severity.
Trial registration: ClinicalTrials.gov NCT04368975.
Keywords: Acute respiratory distress syndrome; Coronavirus; Mechanical ventilation; Outcome.
Conflict of interest statement
The authors declare no conflicts of interest in relation to this manuscript.
Figures
Comment in
-
COVID-19-related and non-COVID-related acute respiratory distress syndrome: two sides of the same coin?Intensive Care Med. 2020 Dec;46(12):2197-2199. doi: 10.1007/s00134-020-06233-w. Epub 2020 Oct 2. Intensive Care Med. 2020. PMID: 33006682 Free PMC article. No abstract available.
References
-
- Wenjie T, Xiang Z, Xuejun M, et al. (2020) A novel coronavirus genome identified in a cluster of pneumonia cases—Wuhan, China 2019−2020. https://weekly.chinacdc.cn/en/article/id/a3907201-f64f-4154-a19e-4253b45.... Accessed 03 July 2020
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
