

Cost-effectiveness of Breast Cancer Screening With Magnetic Resonance Imaging for Women at Familial Risk
- PMID: 32729887
- PMCID: PMC7393584
- DOI: 10.1001/jamaoncol.2020.2922
Cost-effectiveness of Breast Cancer Screening With Magnetic Resonance Imaging for Women at Familial Risk
Abstract
Importance: For women with a 20% or more familial risk of breast cancer without a known BRCA1/2 (BRCA1, OMIM 113705; and BRCA2, OMIM 114480) or TP53 (OMIM 151623) variant, screening guidelines vary substantially, and cost-effectiveness analyses are scarce.
Objective: To assess the cost-effectiveness of magnetic resonance imaging (MRI) screening strategies for women with a 20% or more familial risk for breast cancer without a known BRCA1/2 or TP53 variant.
Design, setting, and participants: In this economic evaluation, conducted from February 1, 2019, to May 25, 2020, microsimulation modeling was used to estimate costs and effectiveness on a lifetime horizon from age 25 years until death of MRI screening among a cohort of 10 million Dutch women with a 20% or more familial risk for breast cancer without a known BRCA1/2 or TP53 variant. A Dutch screening setting was modeled. Most data were obtained from the randomized Familial MRI Screening (FaMRIsc) trial, which included Dutch women aged 30 to 55 years. A health care payer perspective was applied.
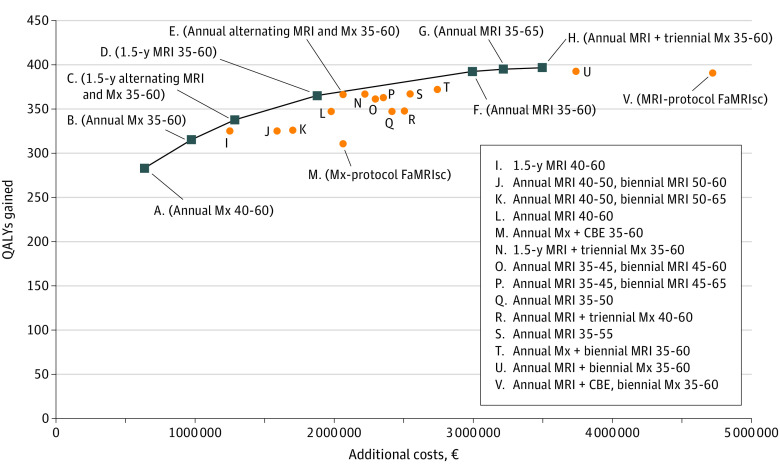
Interventions: Several screening protocols with varying ages and intervals including those of the randomized FaMRIsc trial, consisting of the mammography (Mx) protocol (annual mammography and clinical breast examination) and the MRI protocol (annual MRI and clinical breast examination plus biennial mammography).
Main outcomes and measures: Costs, life-years, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratios (ICERs) were calculated and discounted by 3%. A threshold of €22 000 (US $24 795.87) per QALY was applied.
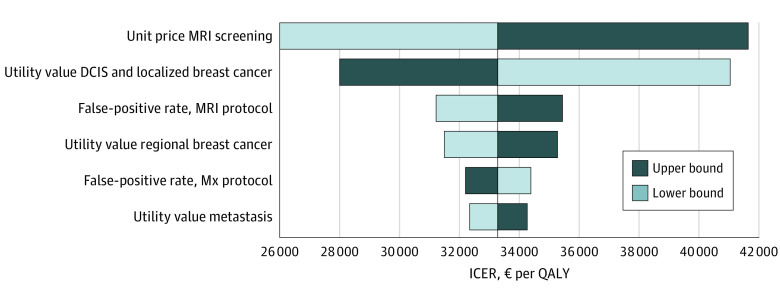
Results: This economic evaluation modeling study estimated that, on a lifetime horizon per 1000 women with the Mx protocol of the FaMRIsc trial, 346 breast cancers would be detected, and 49 women were estimated to die from breast cancer, resulting in 22 885 QALYs and total costs of €7 084 767 (US $7 985 134.61). The MRI protocol resulted in 79 additional QALYs and additional €2 657 266 (US $2 994 964.65). Magnetic resonance imaging performed only every 18 months between the ages of 35 and 60 years followed by the national screening program was considered optimal, with an ICER of €21 380 (US $24 097.08) compared with the previous nondominated strategy in the ranking, when applying the National Institute for Health and Care Excellence threshold. Annual screening alternating MRI and mammography between the ages of 35 and 60 years, followed by the national screening program, gave similar outcomes. Higher thresholds would favor annual MRI screening. The ICER was most sensitive to the unit cost of MRI and the utility value for ductal carcinoma in situ and localized breast cancer.
Conclusions and relevance: This study suggests that MRI screening every 18 months between the ages of 35 and 60 years for women with a family history of breast cancer is cost-effective within the National Institute for Health and Care Excellence threshold for all densities. Higher thresholds would favor annual MRI screening. These outcomes support a change of current screening guidelines for this specific risk group and support MRI screening.
Conflict of interest statement
Figures
Comment in
-
Beyond the AJR: "Cost-Effectiveness of Breast Cancer Screening With Magnetic Resonance Imaging for Women at Familial Risk".AJR Am J Roentgenol. 2021 Jul;217(1):258. doi: 10.2214/AJR.20.25138. Epub 2020 Nov 25. AJR Am J Roentgenol. 2021. PMID: 33236648 No abstract available.
References
-
- oncoline Richtlijn mammacarcinoom (breast cancer national guideline). Accessed January 15, 2019.https://www.oncoline.nl/borstkanker.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
