

Artificial neural networks improve early outcome prediction and risk classification in out-of-hospital cardiac arrest patients admitted to intensive care
- PMID: 32731878
- PMCID: PMC7394679
- DOI: 10.1186/s13054-020-03103-1
Artificial neural networks improve early outcome prediction and risk classification in out-of-hospital cardiac arrest patients admitted to intensive care
Abstract
Background: Pre-hospital circumstances, cardiac arrest characteristics, comorbidities and clinical status on admission are strongly associated with outcome after out-of-hospital cardiac arrest (OHCA). Early prediction of outcome may inform prognosis, tailor therapy and help in interpreting the intervention effect in heterogenous clinical trials. This study aimed to create a model for early prediction of outcome by artificial neural networks (ANN) and use this model to investigate intervention effects on classes of illness severity in cardiac arrest patients treated with targeted temperature management (TTM).
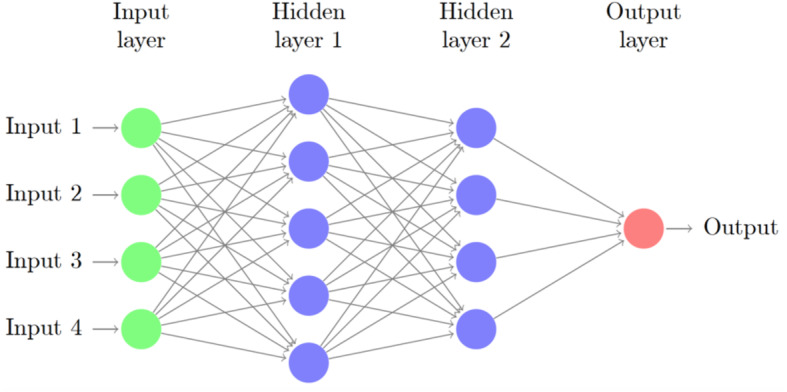
Methods: Using the cohort of the TTM trial, we performed a post hoc analysis of 932 unconscious patients from 36 centres with OHCA of a presumed cardiac cause. The patient outcome was the functional outcome, including survival at 180 days follow-up using a dichotomised Cerebral Performance Category (CPC) scale with good functional outcome defined as CPC 1-2 and poor functional outcome defined as CPC 3-5. Outcome prediction and severity class assignment were performed using a supervised machine learning model based on ANN.
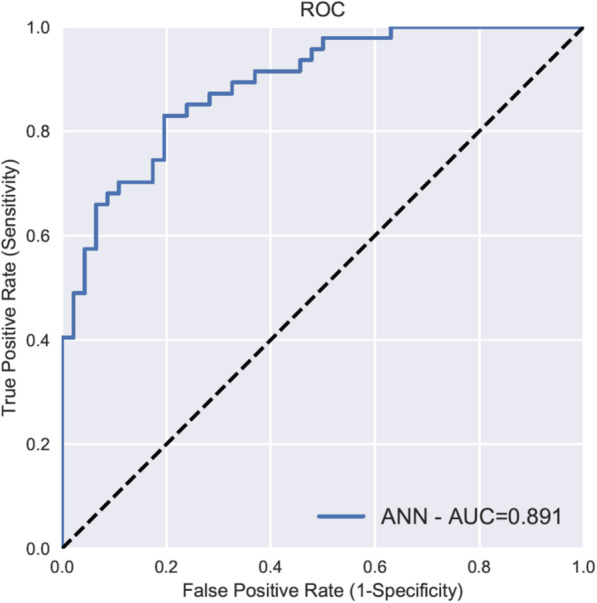
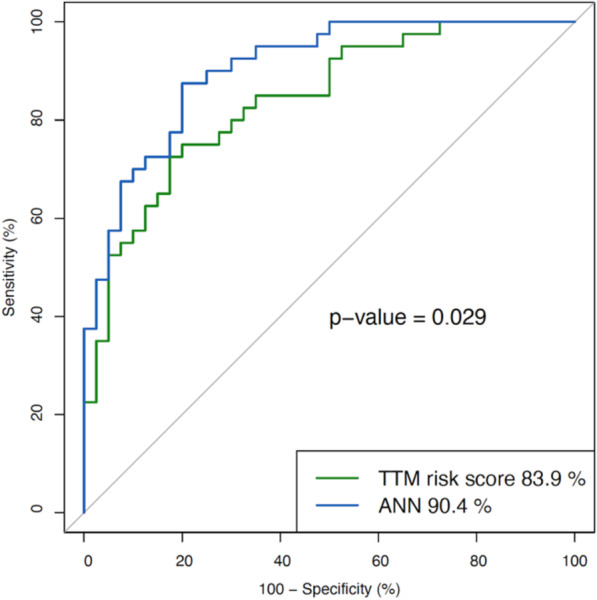
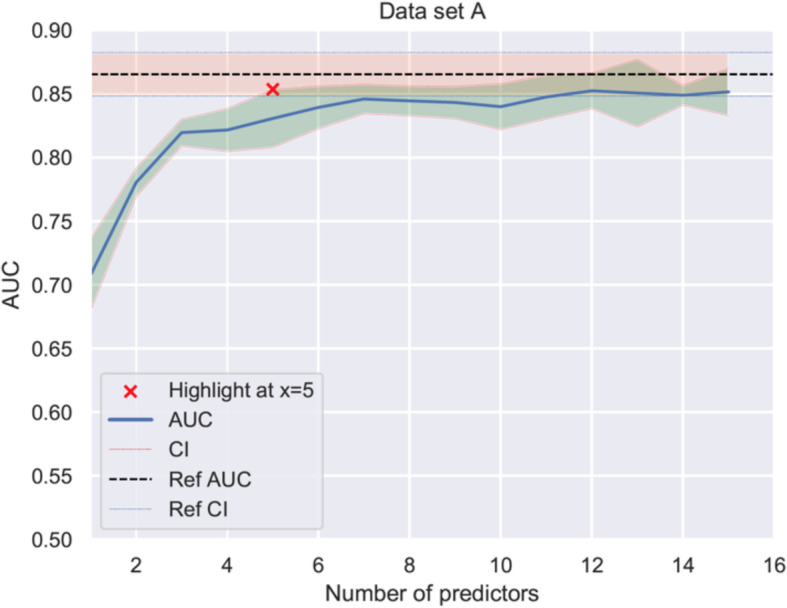
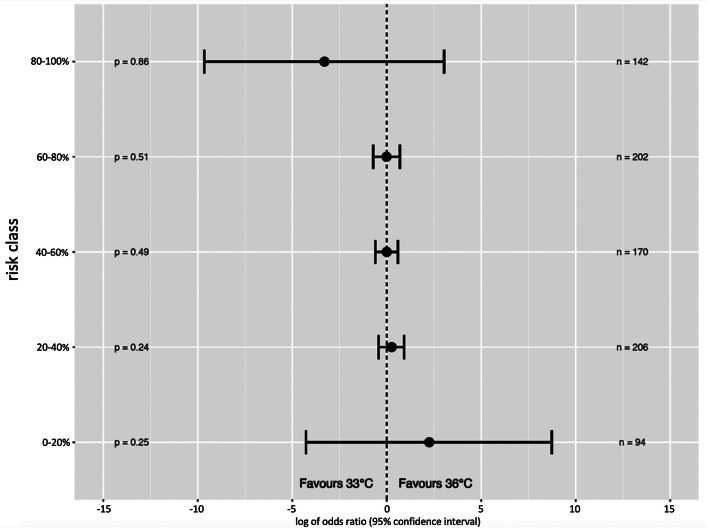
Results: The outcome was predicted with an area under the receiver operating characteristic curve (AUC) of 0.891 using 54 clinical variables available on admission to hospital, categorised as background, pre-hospital and admission data. Corresponding models using background, pre-hospital or admission variables separately had inferior prediction performance. When comparing the ANN model with a logistic regression-based model on the same cohort, the ANN model performed significantly better (p = 0.029). A simplified ANN model showed promising performance with an AUC above 0.852 when using three variables only: age, time to ROSC and first monitored rhythm. The ANN-stratified analyses showed similar intervention effect of TTM to 33 °C or 36 °C in predefined classes with different risk of a poor outcome.
Conclusion: A supervised machine learning model using ANN predicted neurological recovery, including survival excellently, and outperformed a conventional model based on logistic regression. Among the data available at the time of hospitalisation, factors related to the pre-hospital setting carried most information. ANN may be used to stratify a heterogenous trial population in risk classes and help determine intervention effects across subgroups.
Keywords: Artificial intelligence; Artificial neural networks; Cerebral performance category; Critical care; Intensive care; Machine learning; Out-of-hospital cardiac arrest; Prediction; Prognostication.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Predicting neurological outcome after out-of-hospital cardiac arrest with cumulative information; development and internal validation of an artificial neural network algorithm.Crit Care. 2021 Feb 25;25(1):83. doi: 10.1186/s13054-021-03505-9. Crit Care. 2021. PMID: 33632280 Free PMC article.
-
Early predictors of poor outcome after out-of-hospital cardiac arrest.Crit Care. 2017 Apr 13;21(1):96. doi: 10.1186/s13054-017-1677-2. Crit Care. 2017. PMID: 28410590 Free PMC article.
-
Single versus Serial Measurements of Neuron-Specific Enolase and Prediction of Poor Neurological Outcome in Persistently Unconscious Patients after Out-Of-Hospital Cardiac Arrest - A TTM-Trial Substudy.PLoS One. 2017 Jan 18;12(1):e0168894. doi: 10.1371/journal.pone.0168894. eCollection 2017. PLoS One. 2017. PMID: 28099439 Free PMC article. Clinical Trial.
-
Prediction performance of scoring systems after out-of-hospital cardiac arrest: A systematic review and meta-analysis.PLoS One. 2024 Feb 1;19(2):e0293704. doi: 10.1371/journal.pone.0293704. eCollection 2024. PLoS One. 2024. PMID: 38300929 Free PMC article.
-
Targeted temperature management and early neuro-prognostication after cardiac arrest.J Cereb Blood Flow Metab. 2021 Jun;41(6):1193-1209. doi: 10.1177/0271678X20970059. Epub 2021 Jan 14. J Cereb Blood Flow Metab. 2021. PMID: 33444088 Free PMC article. Review.
Cited by
-
Year in Review 2020: Noteworthy Literature in Cardiothoracic Anesthesiology.Semin Cardiothorac Vasc Anesth. 2021 Jun;25(2):94-106. doi: 10.1177/10892532211013614. Epub 2021 May 3. Semin Cardiothorac Vasc Anesth. 2021. PMID: 33938302 Free PMC article.
-
Role of artificial intelligence in predicting neurological outcomes in postcardiac resuscitation.Ann Med Surg (Lond). 2024 Oct 22;86(12):7202-7211. doi: 10.1097/MS9.0000000000002673. eCollection 2024 Dec. Ann Med Surg (Lond). 2024. PMID: 39649879 Free PMC article. Review.
-
Artificial neural network-boosted Cardiac Arrest Survival Post-Resuscitation In-hospital (CASPRI) score accurately predicts outcome in cardiac arrest patients treated with targeted temperature management.Sci Rep. 2022 May 4;12(1):7254. doi: 10.1038/s41598-022-11201-z. Sci Rep. 2022. PMID: 35508580 Free PMC article.
-
Prediction of risk factors for linezolid-induced thrombocytopenia based on neural network model.Front Pharmacol. 2024 Feb 21;15:1292828. doi: 10.3389/fphar.2024.1292828. eCollection 2024. Front Pharmacol. 2024. PMID: 38449807 Free PMC article.
-
Beyond traditional prognostics: integrating RAG-enhanced AtlasGPT and ChatGPT 4.0 into aneurysmal subarachnoid hemorrhage outcome prediction.Neurosurg Rev. 2025 Jan 11;48(1):40. doi: 10.1007/s10143-025-03194-w. Neurosurg Rev. 2025. PMID: 39794551 Free PMC article.
References
-
- Jang DH, Kim J, Jo YH, Lee JH, Hwang JE, Park SM, Lee DK, Park I, Kim D, Chang H. Developing neural network models for early detection of cardiac arrest in emergency department. Am J Emerg Med. 2020;38(1):43-49. - PubMed
-
- Attia ZI, Noseworthy PA, Lopez-Jimenez F, Asirvatham SJ, Deshmukh AJ, Gersh BJ, Carter RE, Yao X, Rabinstein AA, Erickson BJ, et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: a retrospective analysis of outcome prediction. Lancet. 2019;394(10201):861–867. - PubMed
-
- Blomberg SN, Folke F, Ersboll AK, Christensen HC, Torp-Pedersen C, Sayre MR, Counts CR, Lippert FK. Machine learning as a supportive tool to recognize cardiac arrest in emergency calls. Resuscitation. 2019;138:322–329. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
