

Penetrance of Hypertrophic Cardiomyopathy in Sarcomere Protein Mutation Carriers
- PMID: 32731933
- PMCID: PMC7397507
- DOI: 10.1016/j.jacc.2020.06.011
Penetrance of Hypertrophic Cardiomyopathy in Sarcomere Protein Mutation Carriers
Abstract
Background: Predictive genetic screening of relatives of patients with hypertrophic cardiomyopathy (HCM) caused by sarcomere protein (SP) gene mutations is current standard of care, but there are few data on long-term outcomes in mutation carriers without HCM.
Objectives: The aim of this study was to determine the incidence of new HCM diagnosis in SP mutation carriers.
Methods: This was a retrospective analysis of adult and pediatric SP mutation carriers identified during family screening who did not fulfill diagnostic criteria for HCM at first evaluation.
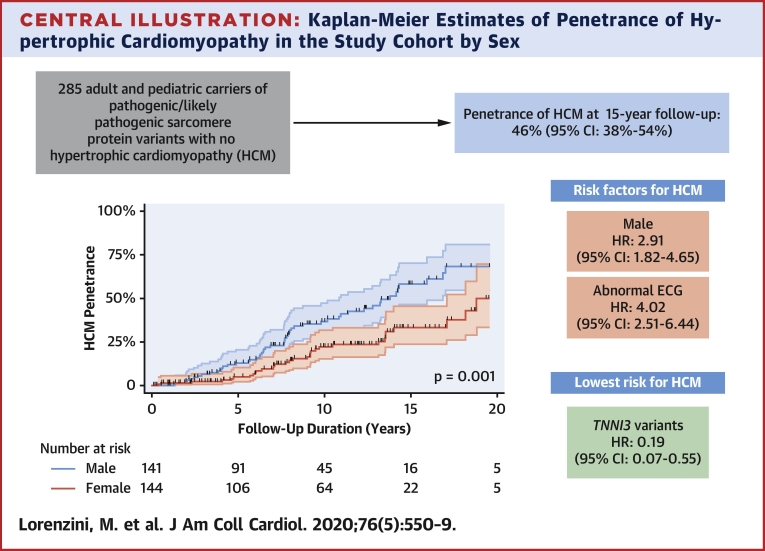
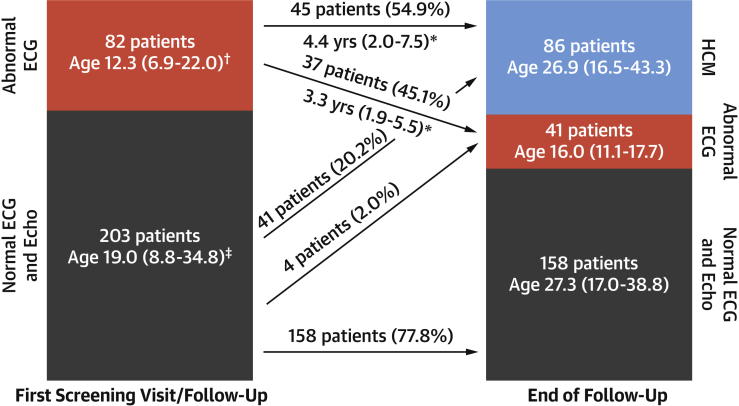
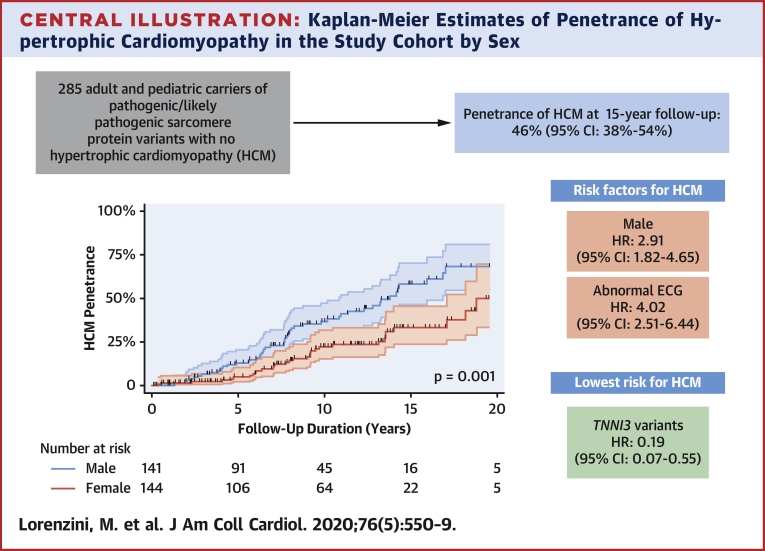
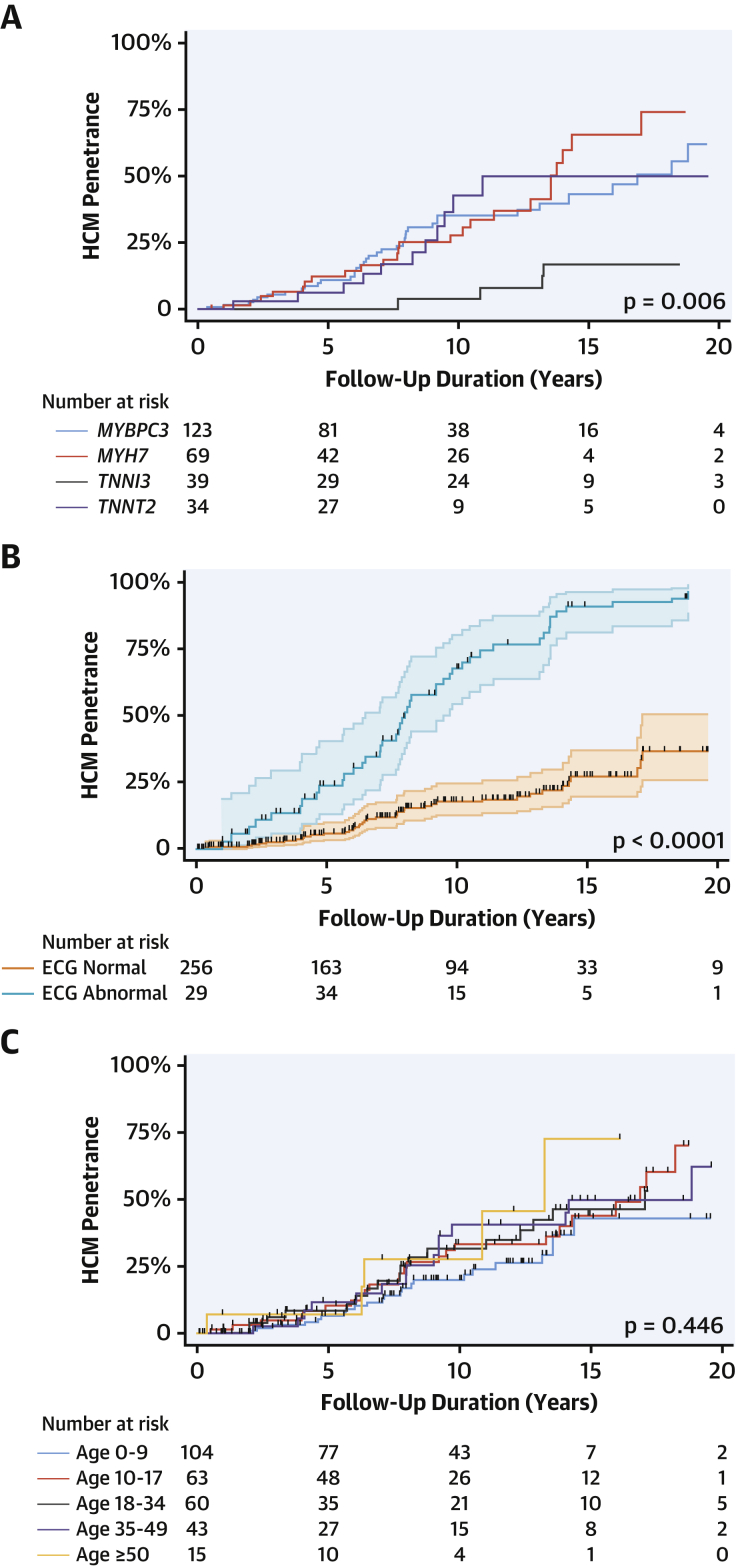
Results: The authors evaluated 285 individuals from 156 families (median age 14.2 years [interquartile range: 6.8 to 31.6 years], 141 [49.5%] male individuals); 145 (50.9%) underwent cardiac magnetic resonance (CMR). Frequency of causal genes was as follows: MYBPC3 n = 123 (43.2%), MYH7 n = 69 (24.2%), TNNI3 n = 39 (13.7%), TNNT2 n = 34 (11.9%), TPM1 n = 9 (3.2%), MYL2 n = 6 (2.1%), ACTC1 n = 1 (0.4%), multiple mutations n = 4 (1.4%). Median follow-up was 8.0 years (interquartile range: 4.0 to 13.3 years) and 86 (30.2%) patients developed HCM; 16 of 50 (32.0%) fulfilled diagnostic criteria on CMR but not echocardiography. Estimated HCM penetrance at 15 years of follow-up was 46% (95% confidence interval [CI]: 38% to 54%). In a multivariable model adjusted for age and stratified for CMR, independent predictors of HCM development were male sex (hazard ratio [HR]: 2.91; 95% CI: 1.82 to 4.65) and abnormal electrocardiogram (ECG) (HR: 4.02; 95% CI: 2.51 to 6.44); TNNI3 variants had the lowest risk (HR: 0.19; 95% CI: 0.07 to 0.55, compared to MYBPC3).
Conclusions: Following a first negative screening, approximately 50% of SP mutation carriers develop HCM over 15 years of follow-up. Male sex and an abnormal ECG are associated with a higher risk of developing HCM. Regular CMR should be considered in long-term screening.
Keywords: ECG; cardiac magnetic resonance; echocardiogram; sex; sudden cardiac death.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Variable Penetrance in Hypertrophic Cardiomyopathy: In Search of the Holy Grail.J Am Coll Cardiol. 2020 Aug 4;76(5):560-562. doi: 10.1016/j.jacc.2020.06.023. J Am Coll Cardiol. 2020. PMID: 32731934 No abstract available.
References
-
- Elliott P.M., Anastasakis A., Borger M.A. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy. Eur Heart J. 2014;35:2733–2779. - PubMed
-
- Vermeer A.M.C., Clur S.-A.A.B., Blom N.A., Wilde A.A.M., Christiaans I. Penetrance of hypertrophic cardiomyopathy in children who are mutation positive. J Pediatr. 2017;188:91–95. - PubMed
-
- Jensen M.K., Havndrup O., Christiansen M. Penetrance of hypertrophic cardiomyopathy in children and adolescents. Circulation. 2013;127:48–54. - PubMed
-
- Maurizi N., Michels M., Rowin E.J. Clinical course and significance of hypertrophic cardiomyopathy without left ventricular hypertrophy. Circulation. 2019;139:830–833. - PubMed
-
- Gray B., Ingles J., Semsarian C. Natural history of genotype positive-phenotype negative patients with hypertrophic cardiomyopathy. Int J Cardiol. 2011;152:258–259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
