

Drug treatments for covid-19: living systematic review and network meta-analysis
- PMID: 32732190
- PMCID: PMC7390912
- DOI: 10.1136/bmj.m2980
Drug treatments for covid-19: living systematic review and network meta-analysis
Erratum in
-
Drug treatments for covid-19: living systematic review and network meta-analysis.BMJ. 2021 Apr 13;373:n967. doi: 10.1136/bmj.n967. BMJ. 2021. PMID: 33849936 No abstract available.
Update in
-
Update to living systematic review on drug treatments for covid-19.BMJ. 2020 Sep 11;370:m3536. doi: 10.1136/bmj.m3536. BMJ. 2020. PMID: 32917676 No abstract available.
-
Update to living systematic review on drug treatments for covid-19.BMJ. 2020 Dec 17;371:m4852. doi: 10.1136/bmj.m4852. BMJ. 2020. PMID: 33334735 No abstract available.
-
Update to living systematic review on drug treatments for covid-19.BMJ. 2021 Mar 31;372:n858. doi: 10.1136/bmj.n858. BMJ. 2021. PMID: 33789885 No abstract available.
Abstract
Objective: To compare the effects of treatments for coronavirus disease 2019 (covid-19).
Design: Living systematic review and network meta-analysis.
Data sources: WHO covid-19 database, a comprehensive multilingual source of global covid-19 literature, up to 3 December 2021 and six additional Chinese databases up to 20 February 2021. Studies identified as of 1 December 2021 were included in the analysis.
Study selection: Randomised clinical trials in which people with suspected, probable, or confirmed covid-19 were randomised to drug treatment or to standard care or placebo. Pairs of reviewers independently screened potentially eligible articles.
Methods: After duplicate data abstraction, a bayesian network meta-analysis was conducted. Risk of bias of the included studies was assessed using a modification of the Cochrane risk of bias 2.0 tool, and the certainty of the evidence using the grading of recommendations assessment, development, and evaluation (GRADE) approach. For each outcome, interventions were classified in groups from the most to the least beneficial or harmful following GRADE guidance.
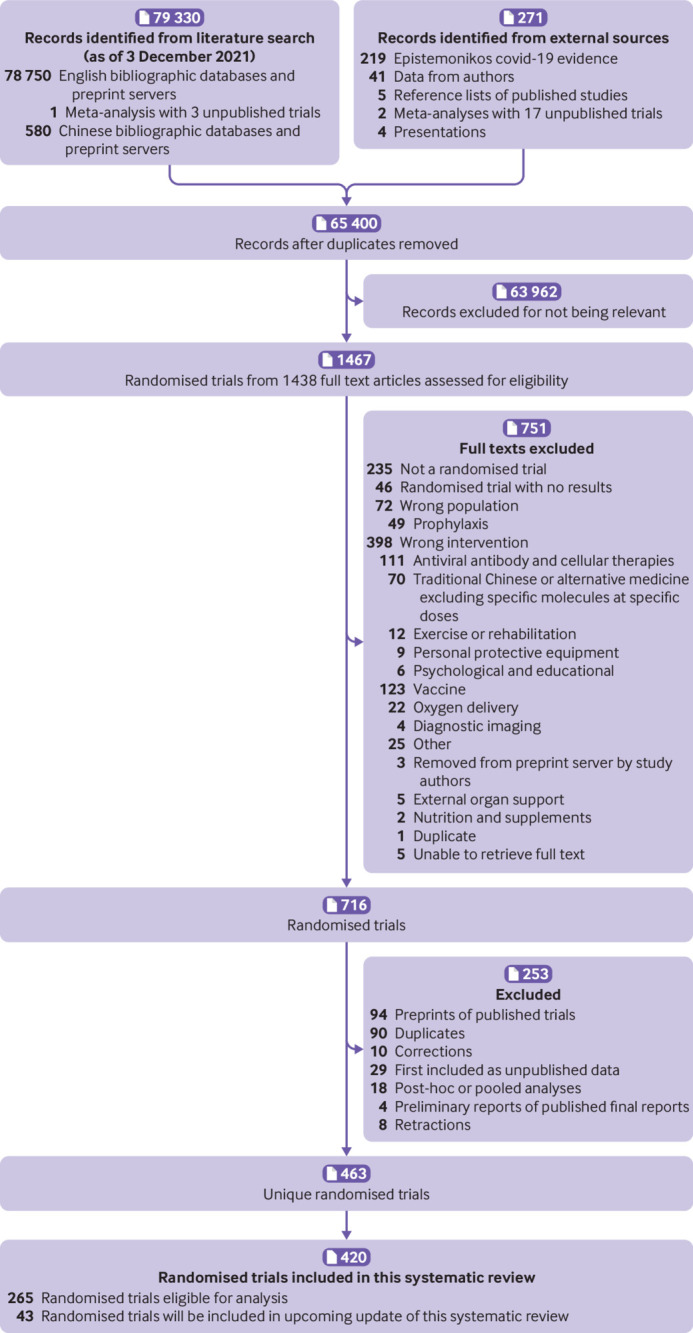
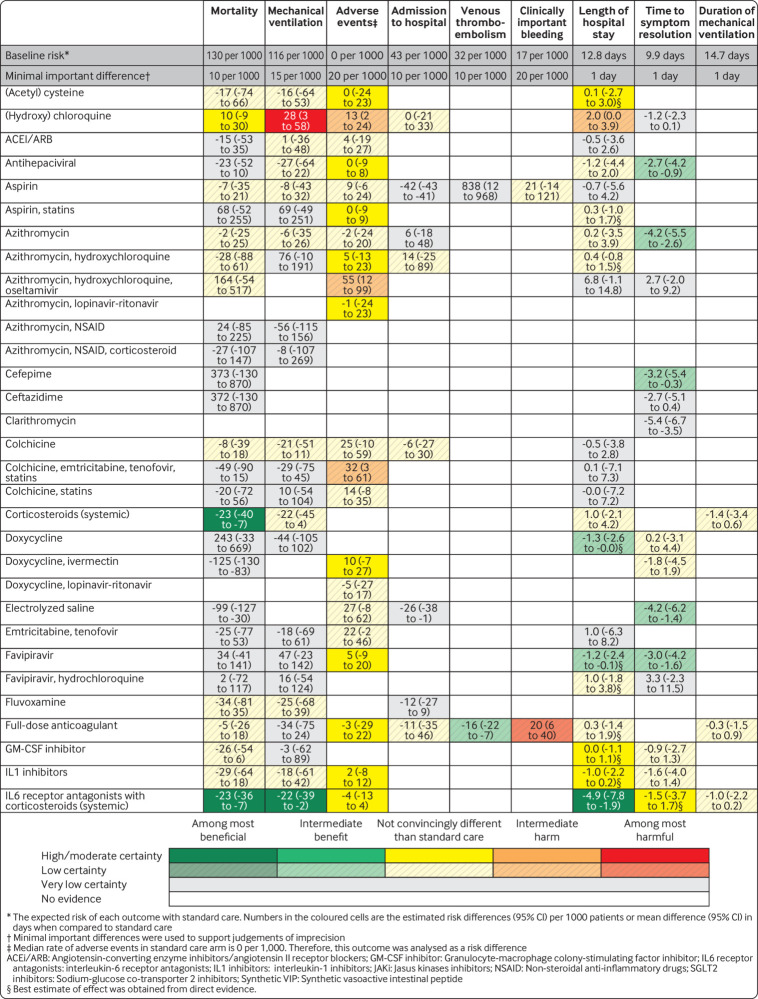
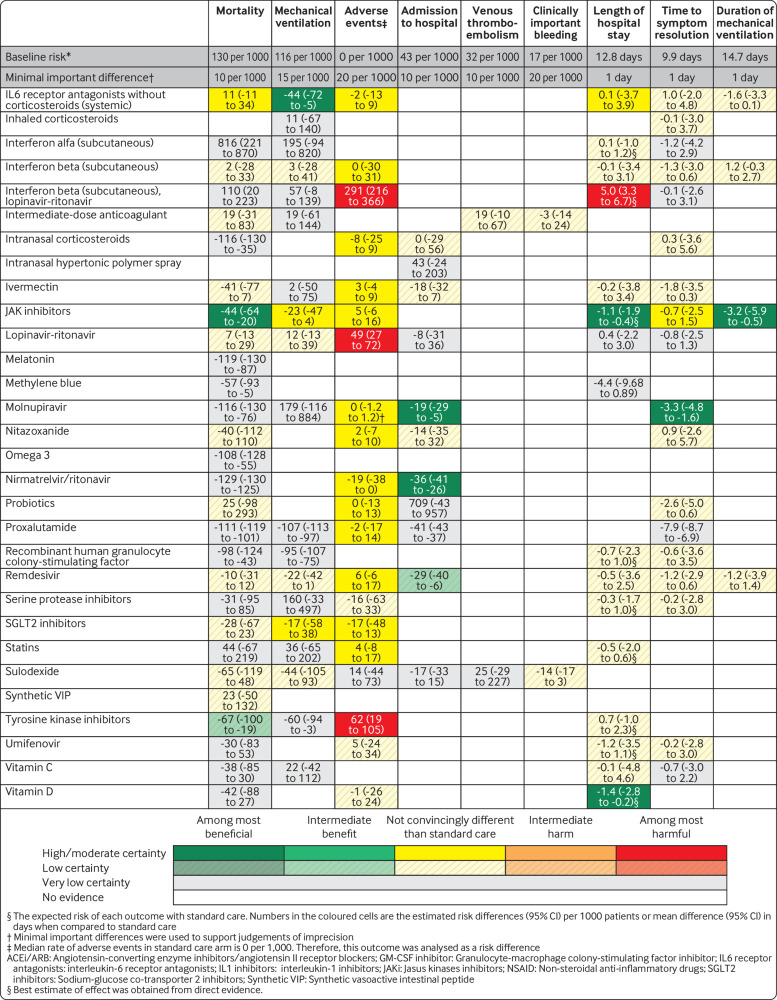
Results: 463 trials enrolling 166 581 patients were included; 267 (57.7%) trials and 89 814 (53.9%) patients are new from the previous iteration; 265 (57.2%) trials evaluating treatments with at least 100 patients or 20 events met the threshold for inclusion in the analyses. Compared with standard care, three drugs reduced mortality in patients with mostly severe disease with at least moderate certainty: systemic corticosteroids (risk difference 23 fewer per 1000 patients, 95% credible interval 40 fewer to 7 fewer, moderate certainty), interleukin-6 receptor antagonists when given with corticosteroids (23 fewer per 1000, 36 fewer to 7 fewer, moderate certainty), and Janus kinase inhibitors (44 fewer per 1000, 64 fewer to 20 fewer, high certainty). Compared with standard care, two drugs probably reduce hospital admission in patients with non-severe disease: nirmatrelvir/ritonavir (36 fewer per 1000, 41 fewer to 26 fewer, moderate certainty) and molnupiravir (19 fewer per 1000, 29 fewer to 5 fewer, moderate certainty). Remdesivir may reduce hospital admission (29 fewer per 1000, 40 fewer to 6 fewer, low certainty). Only molnupiravir had at least moderate quality evidence of a reduction in time to symptom resolution (3.3 days fewer, 4.8 fewer to 1.6 fewer, moderate certainty); several others showed a possible benefit. Several drugs may increase the risk of adverse effects leading to drug discontinuation; hydroxychloroquine probably increases the risk of mechanical ventilation (moderate certainty).
Conclusion: Corticosteroids, interleukin-6 receptor antagonists, and Janus kinase inhibitors probably reduce mortality and confer other important benefits in patients with severe covid-19. Molnupiravir and nirmatrelvir/ritonavir probably reduce admission to hospital in patients with non-severe covid-19.
Systematic review registration: This review was not registered. The protocol is publicly available in the supplementary material.
Readers' note: This article is a living systematic review that will be updated to reflect emerging evidence. Updates may occur for up to two years from the date of original publication. This is the fifth version of the original article published on 30 July 2020 (BMJ 2020;370:m2980), and previous versions can be found as data supplements. When citing this paper please consider adding the version number and date of access for clarity.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Canadian Institutes of Health Research; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Update to living systematic review on drug treatments for covid-19.BMJ. 2022 Jul 13;378:o1717. doi: 10.1136/bmj.o1717. BMJ. 2022. PMID: 35830977 No abstract available.
References
-
- John Hopkins University. Coronavirus Resource Center 2020 https://coronavirus.jhu.edu/map.html.
-
- Cytel. Global coronavirus COVID-19 clinical trial tracker. 2020 https://www.covid19-trials.org/.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous