

What Influences Patient Satisfaction after TKA? A Qualitative Investigation
- PMID: 32732567
- PMCID: PMC7371044
- DOI: 10.1097/CORR.0000000000001284
What Influences Patient Satisfaction after TKA? A Qualitative Investigation
Abstract
Background: Patient satisfaction is a common measure of the success of an orthopaedic intervention. However, there is poor understanding of what satisfaction means to patients or what influences it.
Questions/purposes: Using qualitative study methodology in patients undergoing TKA, we asked: (1) What does it mean to be satisfied after TKA? (2) What factors influence satisfaction levels after TKA?
Methods: People in a hospital registry who had completed 12-month follow-up questionnaires and were not more than 18 months post-TKA at the time of sampling were eligible (n = 121). To recruit a sample that provided insight into a range of TKA experiences, we divided eligible candidates on the registry into quadrants based on their responder status and satisfaction level. A responder was an individual who experienced a clinically meaningful change in pain and/or function on the WOMAC according to the Outcome Measures in Rheumatology-Osteoarthritis Research Society International (OMERACT-OARSI) responder criteria. Individuals were considered satisfied unless they indicated somewhat dissatisfied or very dissatisfied for one or more of the four items on the Self-Administered Patient Satisfaction Scale. From the resulting quadrants: responder satisfied, nonresponder satisfied, nonresponder dissatisfied, responder dissatisfied, we identified men and women with a range of ages and invited them to participate (n = 85). The final sample (n = 40), consisted of 10 responder satisfied, nine nonresponder satisfied, eight nonresponder dissatisfied, and 13 responder dissatisfied; 71% were women, with a mean age of 71 ± 7 years and a mean time since TKA surgery of 17 ± 2 months (range 13 to 25 months). Interview transcripts were analyzed by looking for factors in the participants' narrative that appeared to underscore their level of satisfaction and attaching inductive (data-derived, rather than a priori derived) codes to relevant sections of text. Coded data from participants who reported high and low levels of satisfaction were compared/contrasted and emerging patterns were mapped into a conceptual model. Recruitment continued until no new information was uncovered in data analysis of subsequent interviews, signalling to the researchers that further interviews would not change the key themes identified and data collection could cease.
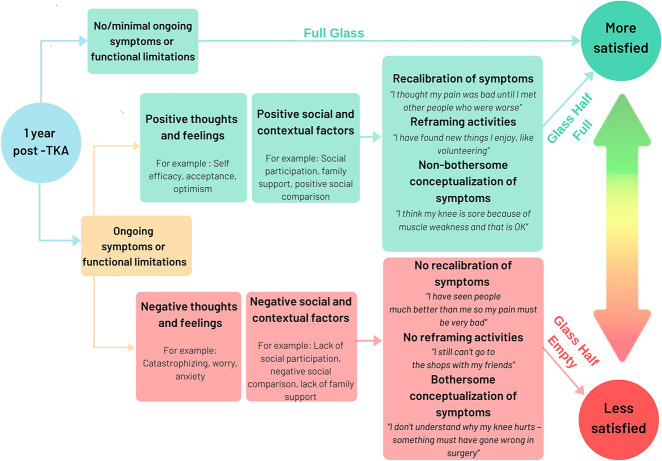
Results: In those with high satisfaction levels, satisfaction was conceptualized as an improvement in pain and function. In those with low satisfaction levels, rather than an improvement, satisfaction was conceptualized as completely resolving all symptoms and functional limitations. In addition, we identified three pathways through which participants reached different levels of low and high satisfaction: (1) The full-glass pathway, characterized by no or minimal ongoing symptoms and functional deficits, which consistently led to high levels of satisfaction; (2) the glass-half-full pathway, characterized by ongoing symptoms and functional limitations, which led to high satisfaction; and (3) the glass-half-empty pathway, also characterized by ongoing symptoms and functional limitations, which led to low satisfaction levels. The latter two pathways were mediated by three core mechanisms (recalibration, reframing valued activities, and reconceptualization) influenced either positively or negatively by (1) a persons' thoughts and feelings such as optimism, self-efficacy, pain catastrophizing, external locus of control; and (2) social and contextual factors such as fulfilment of social roles, therapeutic alliance, lack of family/social support.
Conclusions: This qualitative study suggests that for preoperative patients in whom unrealistically high hopes for complete symptom resolution and restoration of functional capacity persists, it may be appropriate to direct them away from TKA due to the risk of low satisfaction. For postoperative patients troubled by ongoing symptoms or functional limitations, clinicians may improve levels of satisfaction by targeting the three core mechanisms (recalibration, reframing valued activities, and reconceptualization) through addressing modifiable negative thoughts and feelings in interventions such as psychology or psychotherapy; and negative social and contextual factors by promoting a strong therapeutic alliance and engagement in community activities. Given that these factors may be identifiable preoperatively, future research is needed to explore if and how addressing them preoperatively may improve satisfaction post-TKA.
Level of evidence: Level IV, therapeutic study.
Conflict of interest statement
Each author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: What Influences Patient Satisfaction after TKA? A Qualitative Investigation.Clin Orthop Relat Res. 2020 Aug;478(8):1867-1869. doi: 10.1097/CORR.0000000000001363. Clin Orthop Relat Res. 2020. PMID: 32732568 Free PMC article. No abstract available.
References
-
- Ali A, Lindstrand A, Sundberg M, Flivik G. Preoperative Anxiety and Depression Correlate With Dissatisfaction After Total Knee Arthroplasty: A Prospective Longitudinal Cohort Study of 186 Patients, With 4-Year Follow-Up. J Arthroplasty. 2017;32:767-770. - PubMed
-
- Barclay-Goddard R, Epstein JD, Mayo NE. Response shift: a brief overview and proposed research priorities. Qual Life Res. 2009;18:335-346. - PubMed
-
- Batbaatar E, Dorjdagva J, Luvsannyam A, Amenta P. Conceptualisation of patient satisfaction: a systematic narrative literature review. Perspect Public Health. 2015;135:243-250. - PubMed
-
- Batbaatar E, Dorjdagva J, Luvsannyam A, Savino MM, Amenta P. Determinants of patient satisfaction: a systematic review. Perspect Public Health. 2017;137:89-101. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
