

Capnovolumetry in combination with clinical history for the diagnosis of asthma and COPD
- PMID: 32732930
- PMCID: PMC7393160
- DOI: 10.1038/s41533-020-00190-z
Capnovolumetry in combination with clinical history for the diagnosis of asthma and COPD
Abstract
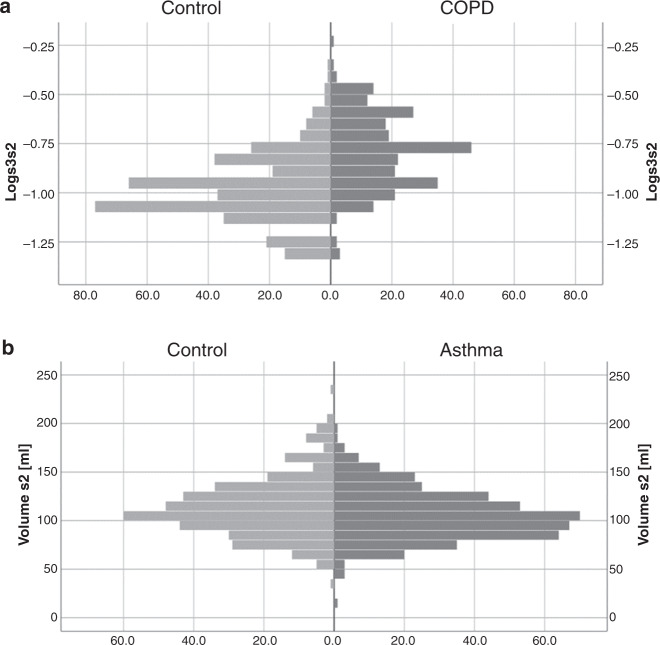
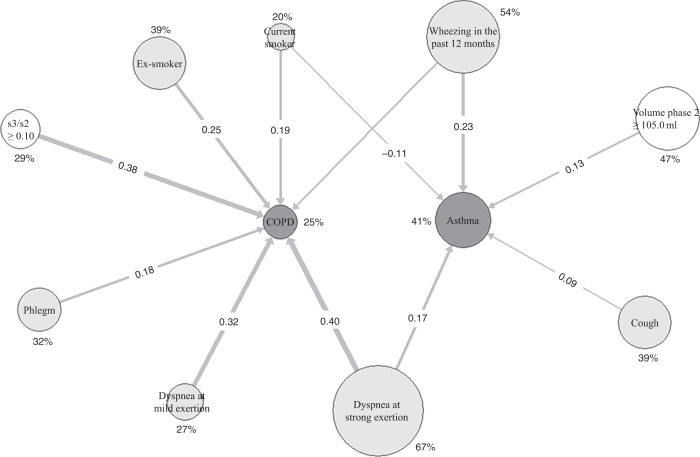
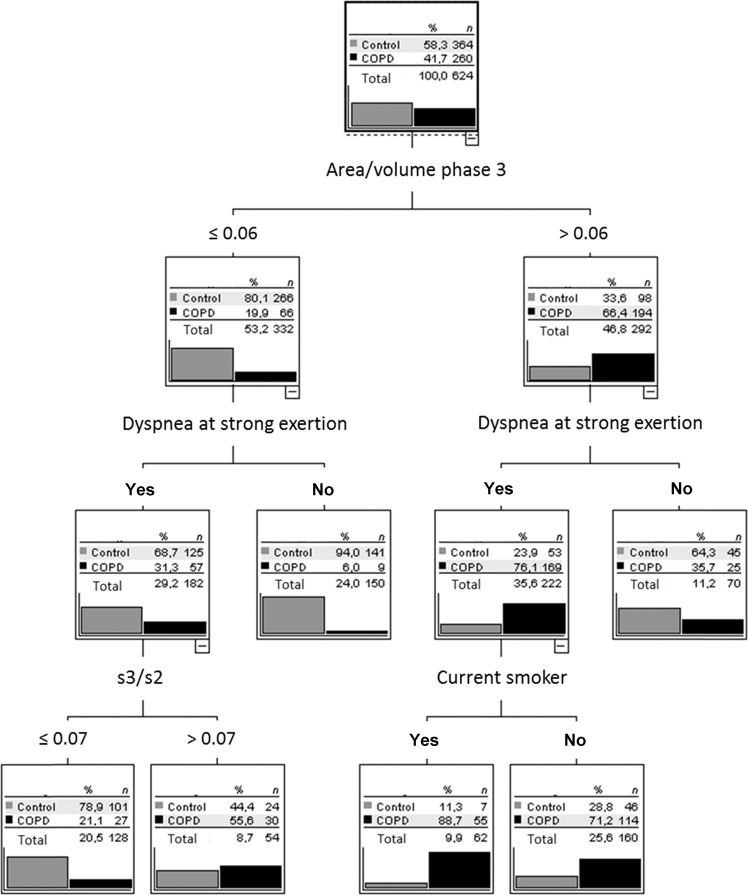
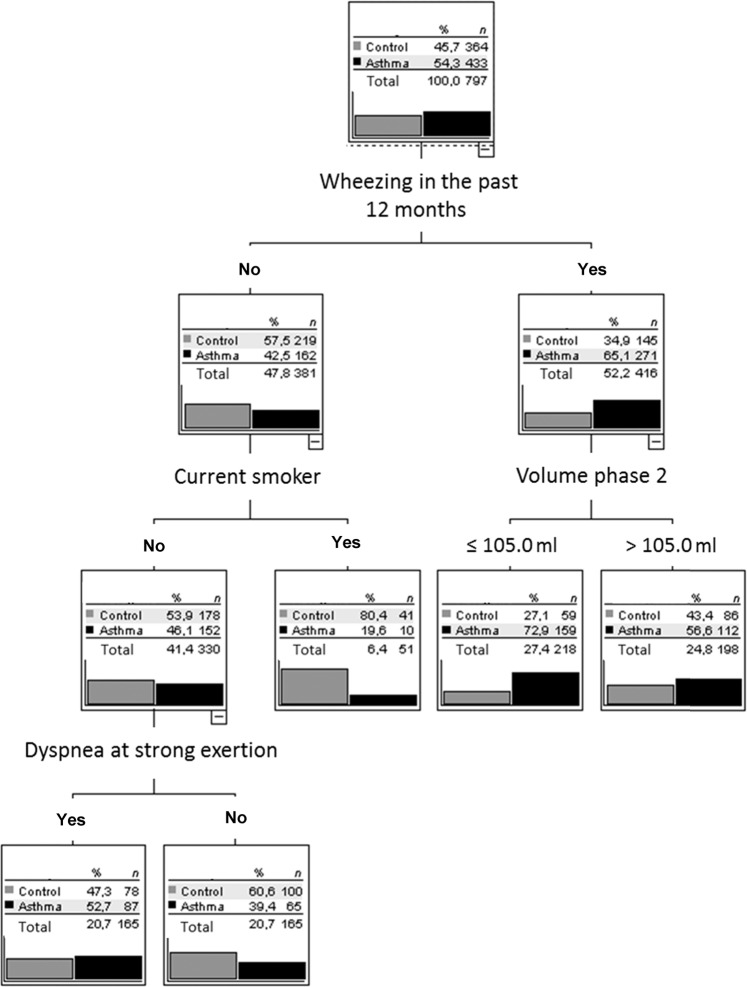
Capnovolumetry performed during resting ventilation is an easily applicable diagnostic tool sensitive to airway obstruction. In the present analysis, we investigated in which way capnovolumetric parameters can be combined with basic anamnestic information to support the diagnosis of asthma and COPD. Among 1400 patients of a previous diagnostic study, we selected 1057 patients with a diagnosis of asthma (n = 433), COPD (n = 260), or without respiratory disease (n = 364). Besides performing capnovolumetry, patients answered questions on symptoms and smoking status. Logistic regression analysis, single decision trees (CHAID), and ensembles of trees (random forest) were used to identify diagnostic patterns of asthma and COPD. In the random forest approach, area/volume of phase 3, dyspnea upon strong exertion, s3/s2, and current smoking were identified as relevant parameters for COPD vs control. For asthma vs control, they were wheezing, volume of phase 2, current smoking, and dyspnea at strong exertion. For COPD vs asthma, s3/s2 was the primary criterion, followed by current smoking and smoking history. These parameters were also identified as relevant in single decision trees. Regarding the diagnosis of asthma vs control, COPD vs control, and COPD vs asthma, the area under the curve was 0.623, 0.875, and 0.880, respectively, in the random forest approach. Our results indicate that for the diagnosis of asthma and COPD capnovolumetry can be combined with basic anamnestic information in a simple, intuitive, and efficient manner. As capnovolumetry requires less cooperation from the patient than spirometry, this approach might be helpful for clinical practice.
Conflict of interest statement
The Institute of General Practice and Health Services Research (Munich, Germany) received a grant from Ganshorn Medizin Electronic GmbH (Niederlauer, Germany) during the conduct of the study. The funders did not play any role in the design of the study, data evaluation and interpretation of the results.
Figures

References
-
- Ponto S, Aufderhaar M, Bauer J. Kapnovolumetrie als mitarbeitsfreie methode für die diagnostik und überwachung von COPD. Pneumologie. 2016;70:826–830. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
