

Emerging evidence of a COVID-19 thrombotic syndrome has treatment implications
- PMID: 32733003
- PMCID: PMC7391481
- DOI: 10.1038/s41584-020-0474-5
Emerging evidence of a COVID-19 thrombotic syndrome has treatment implications
Abstract
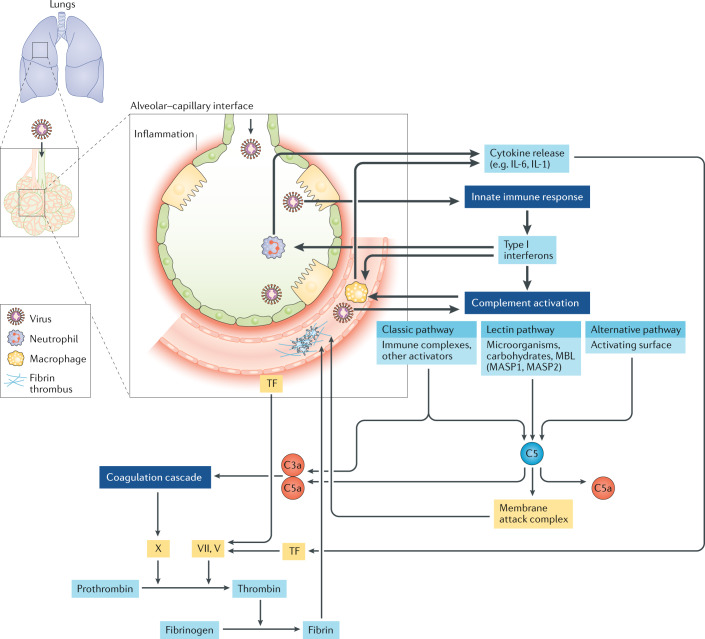
Reports of widespread thromboses and disseminated intravascular coagulation (DIC) in patients with coronavirus disease 19 (COVID-19) have been rapidly increasing in number. Key features of this disorder include a lack of bleeding risk, only mildly low platelet counts, elevated plasma fibrinogen levels, and detection of both severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and complement components in regions of thrombotic microangiopathy (TMA). This disorder is not typical DIC. Rather, it might be more similar to complement-mediated TMA syndromes, which are well known to rheumatologists who care for patients with severe systemic lupus erythematosus or catastrophic antiphospholipid syndrome. This perspective has critical implications for treatment. Anticoagulation and antiviral agents are standard treatments for DIC but are gravely insufficient for any of the TMA disorders that involve disorders of complement. Mediators of TMA syndromes overlap with those released in cytokine storm, suggesting close connections between ineffective immune responses to SARS-CoV-2, severe pneumonia and life-threatening microangiopathy.
Conflict of interest statement
J.T.M. declares that she has received consulting fees from Alexion Pharmaceuticals. The other authors declare no competing interests.
Figures
References
-
- Zheng R, et al. Clinical characteristics of 161 cases of corona virus disease 2019 (COVID-19) in Changsha. Eur. Rev. Med. Pharmacol. Sci. 2020;24:3404–3410. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
