

Extracorporeal Cardiopulmonary Resuscitation (ECPR) for Out-of-Hospital Cardiac Arrest due to Pulseless Ventricular Tachycardia/Fibrillation
- PMID: 32733171
- PMCID: PMC7382749
- DOI: 10.1155/2020/6939315
Extracorporeal Cardiopulmonary Resuscitation (ECPR) for Out-of-Hospital Cardiac Arrest due to Pulseless Ventricular Tachycardia/Fibrillation
Abstract
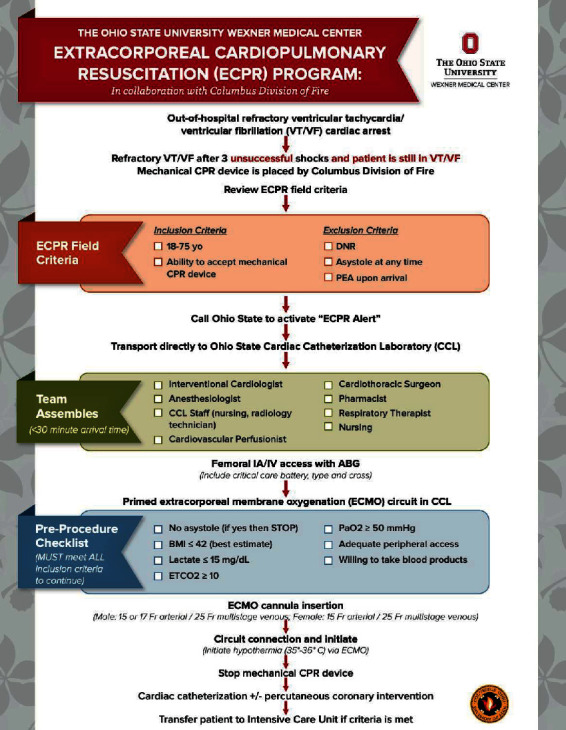
Background: Survival rates for out-of-hospital cardiac arrest are very low and neurologic recovery is poor. Innovative strategies have been developed to improve outcomes. A collaborative extracorporeal cardiopulmonary resuscitation (ECPR) program for out-of-hospital refractory pulseless ventricular tachycardia (VT) and/or ventricular fibrillation (VF) has been developed between The Ohio State University Wexner Medical Center and Columbus Division of Fire.
Methods: From August 15, 2017, to June 1, 2019, there were 86 patients that were evaluated in the field for cardiac arrest in which 42 (49%) had refractory pulseless VT and/or VF resulting from different underlying pathologies and were placed on an automated cardiopulmonary resuscitation device; from these 42 patients, 16 (38%) met final inclusion criteria for ECPR and were placed on extracorporeal membrane oxygenation (ECMO) in the cardiac catheterization laboratory (CCL).
Results: From the 16 patients who underwent ECPR, 4 (25%) survived to hospital discharge with cerebral perfusion category 1 or 2. Survivors tended to be younger (48.0 ± 16.7 vs. 59.3 ± 12.7 years); however, this difference was not statistically significant (p=0.28) likely due to a small number of patients. Overall, 38% of patients underwent percutaneous coronary intervention (PCI). No significant difference was found between survivors and nonsurvivors in emergency medical services dispatch to CCL arrival time, lactate in CCL, coronary artery disease severity, undergoing PCI, and pre-ECMO PaO2, pH, and hemoglobin. Recovery was seen in different underlying pathologies.
Conclusion: ECPR for out-of-hospital refractory VT/VF cardiac arrest demonstrated encouraging outcomes. Younger patients may have a greater chance of survival, perhaps the need to be more aggressive in this subgroup of patients.
Copyright © 2020 Konstantinos Dean Boudoulas et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
