

Efficacy and Safety of Intravenous Thrombolysis on Acute Branch Atheromatous Disease: A Retrospective Case-Control Study
- PMID: 32733357
- PMCID: PMC7358343
- DOI: 10.3389/fneur.2020.00581
Efficacy and Safety of Intravenous Thrombolysis on Acute Branch Atheromatous Disease: A Retrospective Case-Control Study
Abstract
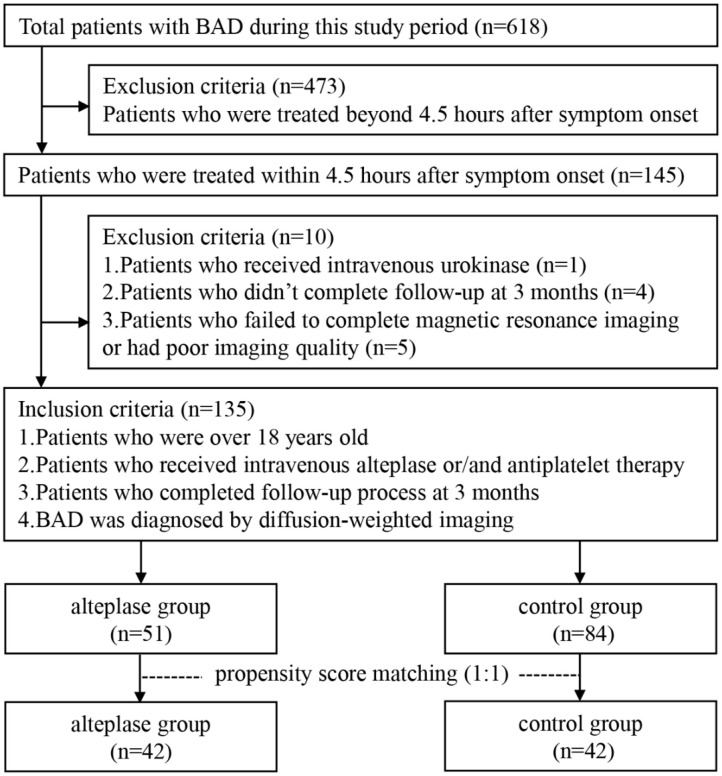
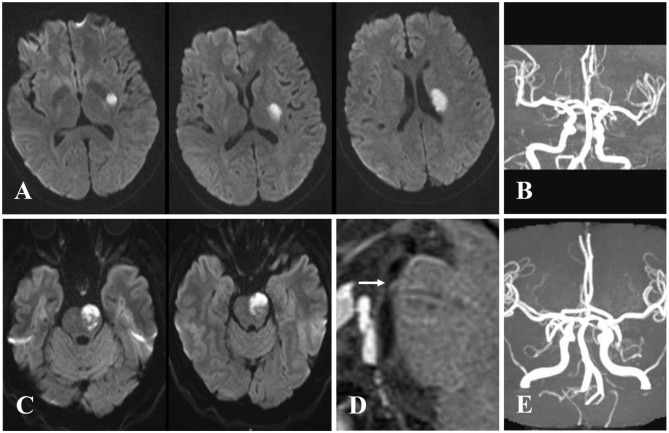
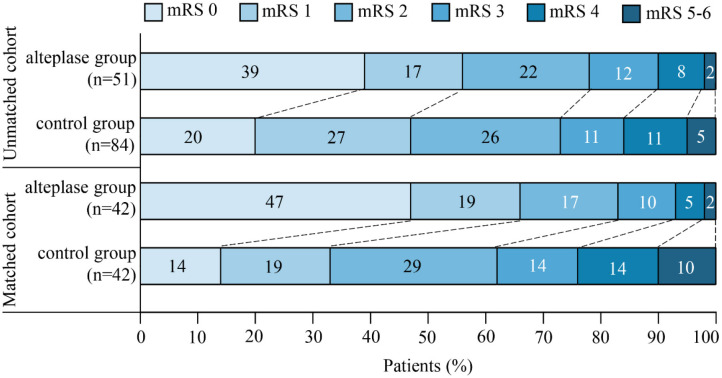
Background and Objective: Branch atheromatous disease (BAD) is distinctive from large-artery atherosclerosis and small-vessel disease, which is single subcortical infarction caused by the occlusion of perforator's orifice. This study aimed to indicate whether intravenous thrombolysis (IVT) with alteplase could prevent early neurological deterioration (END) and improve functional outcome for patients with BAD within 4.5 h after symptom onset. Methods: We retrospectively analyzed data collected from patients with BAD who were admitted to our hospital from January 2015 to August 2019. To investigate the efficacy and safety of IVT, subjects were classified into alteplase and control groups. A propensity score matching analysis was performed to control substantial heterogeneity of subgroup. The coprimary outcomes were END that is defined as an increase of ≥2 points in the National Institutes of Health Stroke Scale (NIHSS) score within 7 days after stroke, and favorable outcome at 3 months after stroke that defined by a score of 0-1 point on the modified Rankin scale (mRS). Results: A total of 135 patients were eventually enrolled in this study (n = 51 for the alteplase group and n = 84 for the control group). Additionally, 42 pairs of subjects were successfully matched by propensity score matching. Intravenous alteplase within 4.5 h after stroke onset reduced the incidence of END [unadjusted odds ratio (OR), 3.32; 95% confidence interval (CI), 1.06-10.37] and improved the clinical outcome at 3 months after stroke, with more patients achieving favorable functional prognosis (mRS, 0-1 point; unadjusted OR, 0.25; 95% CI, 0.10-0.62). Patients in the alteplase group were more likely to be independent (mRS, 0-2 points) at 3 months after stroke (unadjusted OR, 0.33; 95% CI, 0.12-0.90). The rate of death or dependence (mRS, ≥4 points) in the alteplase group was also markedly lower than that in the control group (unadjusted OR, 4.06; 95% CI, 1.03-16.02). Conclusion: Our findings indicated that intravenous thrombolysis may be a safe and effective therapy for patients with BAD.
Keywords: acute stroke; antiplatelet treatment; branch atheromatous disease; early neurological deterioration; intravenous thrombolysis; propensity score matching.
Copyright © 2020 Wu, Liu, Nie, Kang, Wang, Sun, Li, Liu and Mei.
Figures
References
LinkOut - more resources
Full Text Sources
Medical
Research Materials