

Tuberous Sclerosis Complex-Associated Neuropsychiatric Disorders (TAND): New Findings on Age, Sex, and Genotype in Relation to Intellectual Phenotype
- PMID: 32733359
- PMCID: PMC7358578
- DOI: 10.3389/fneur.2020.00603
Tuberous Sclerosis Complex-Associated Neuropsychiatric Disorders (TAND): New Findings on Age, Sex, and Genotype in Relation to Intellectual Phenotype
Abstract
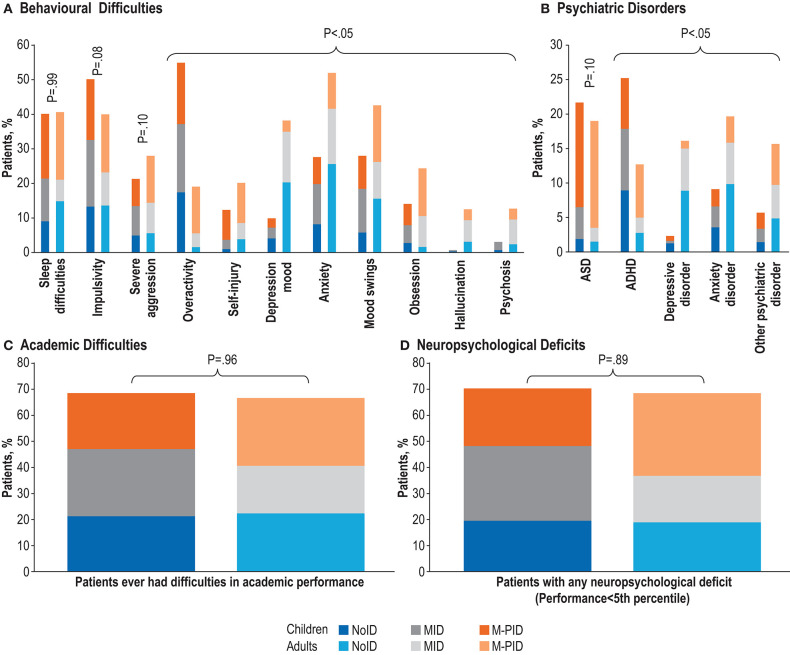
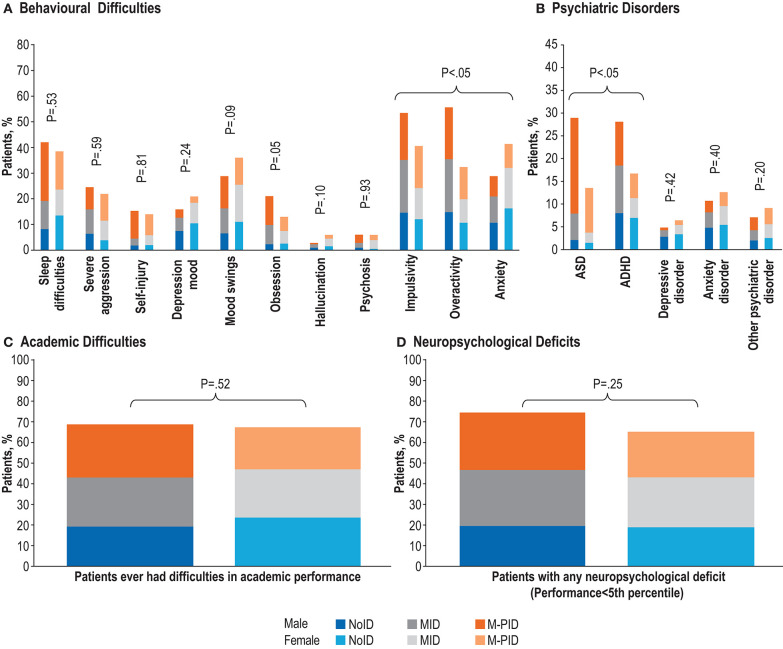
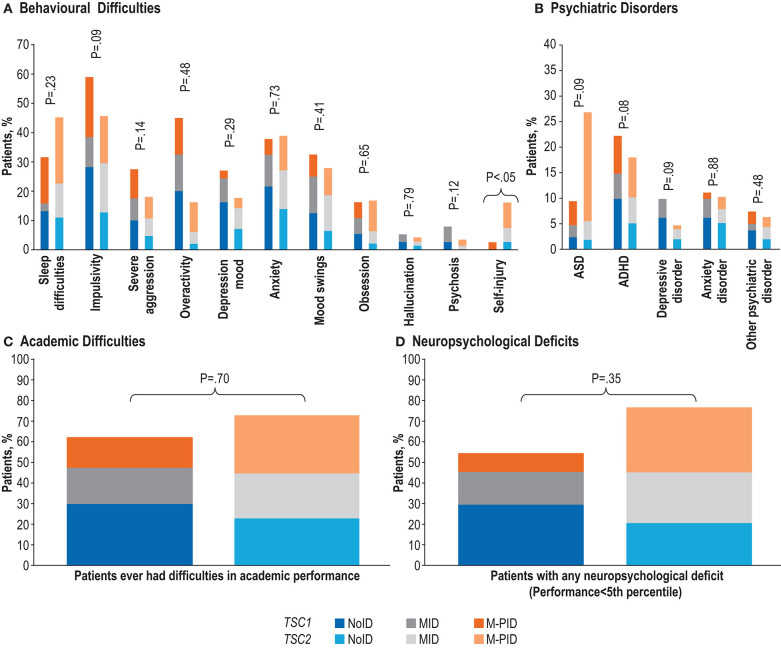
Background: Knowledge is increasing about TSC-Associated Neuropsychiatric Disorders (TAND), but little is known about the potentially confounding effects of intellectual ability (IA) on the rates of TAND across age, sex, and genotype. We evaluated TAND in (a) children vs. adults, (b) males vs. females, and (c) TSC1 vs. TSC2 mutations, after stratification for levels of IA, in a large, international cohort. Methods: Individuals of any age with a documented visit for TSC in the 12 months prior to enrolment were included. Frequency and percentages of baseline TAND manifestations were presented by categories of IA (no intellectual disability [ID, intelligence quotient (IQ)>70]; mild ID [IQ 50-70]; moderate-to-profound ID [IQ<50]). Chi-square tests were used to test associations between ID and TAND manifestations. The association between TAND and age (children vs. adults), sex (male vs. female), and genotype (TSC1 vs. TSC2) stratified by IA levels were examined using the Cochran-Mantel-Haenszel tests. Results: Eight hundred and ninety four of the 2,211 participants had formal IQ assessments. There was a significant association (P < 0.05) between levels of IA and the majority of TAND manifestations, except impulsivity (P = 0.12), overactivity (P = 0.26), mood swings (P = 0.08), hallucinations (P = 0.20), psychosis (P = 0.06), depressive disorder (P = 0.23), and anxiety disorder (P = 0.65). Once controlled for IA, children had higher rates of overactivity, but most behavioral difficulties were higher in adults. At the psychiatric level, attention deficit hyperactivity disorder (ADHD) was seen at higher rates in children while anxiety and depressive disorders were observed at higher rates in adults. Compared to females, males showed significantly higher rates of impulsivity and overactivity, as well as autism spectrum disorder (ASD) and ADHD. No significant age or sex differences were observed for academic difficulties or neuropsychological deficits. After controlling for IA no genotype-TAND associations were observed, except for higher rates of self-injury in individuals with TSC2 mutations. Conclusions: Findings suggest IA as risk marker for most TAND manifestations. We provide the first evidence of male preponderance of ASD and ADHD in individuals with TSC. The study also confirms the association between TSC2 and IA but, once controlling for IA, disproves the previously reported TSC2 association with ASD and with most other TAND manifestations.
Keywords: TAND profile; TOSCA; TSC-associated neuropsychiatric disorders; intelligence quotient; tuberous sclerosis complex.
Copyright © 2020 de Vries, Belousova, Benedik, Carter, Cottin, Curatolo, Dahlin, D'Amato, Beaure d'Augères, Ferreira, Feucht, Fladrowski, Hertzberg, Jozwiak, Lawson, Macaya, Marques, Nabbout, O'Callaghan, Qin, Sander, Sauter, Shah, Takahashi, Touraine, Youroukos, Zonnenberg, Kingswood and Jansen.
Figures
References
-
- Waltereit R, Feucht M, de Vries MC, Huemer J, Roessner V, de Vries PJ. Neuropsychiatric manifestations in Tuberous Sclerosis Complex (TSC): diagnostic guidelines, TAND concept and therapy with mTOR inhibitors. Z Kinder Jugendpsychiatr Psychother. (2019) 47:139–53. 10.1024/1422-4917/a000604 - DOI - PubMed
LinkOut - more resources
Full Text Sources