

Impact of Rescheduling a Missed Hemodialysis Treatment on Clinical Outcomes
- PMID: 32734224
- PMCID: PMC7380431
- DOI: 10.1016/j.xkme.2019.10.007
Impact of Rescheduling a Missed Hemodialysis Treatment on Clinical Outcomes
Abstract
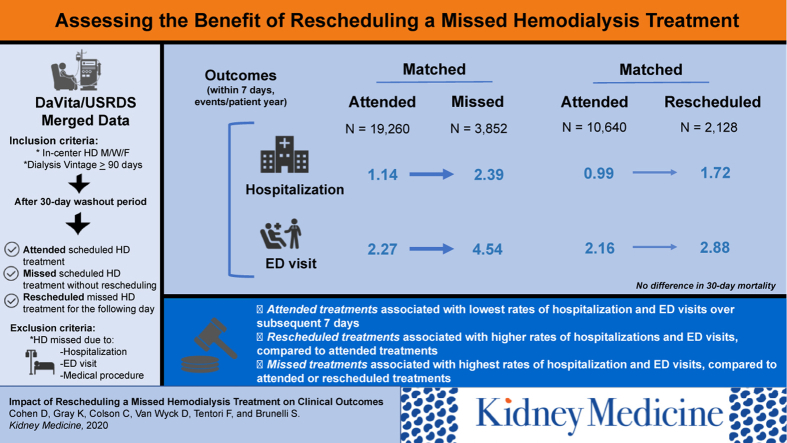
Rationale & objective: Among patients treated with in-center hemodialysis (HD), missed treatments are associated with higher subsequent rates of hospitalization and other adverse outcomes compared with attending treatment. The objective of this study was to determine whether and to what degree attending a rescheduled treatment on the day following a missed treatment ameliorates these risks.
Study design: Retrospective, observational.
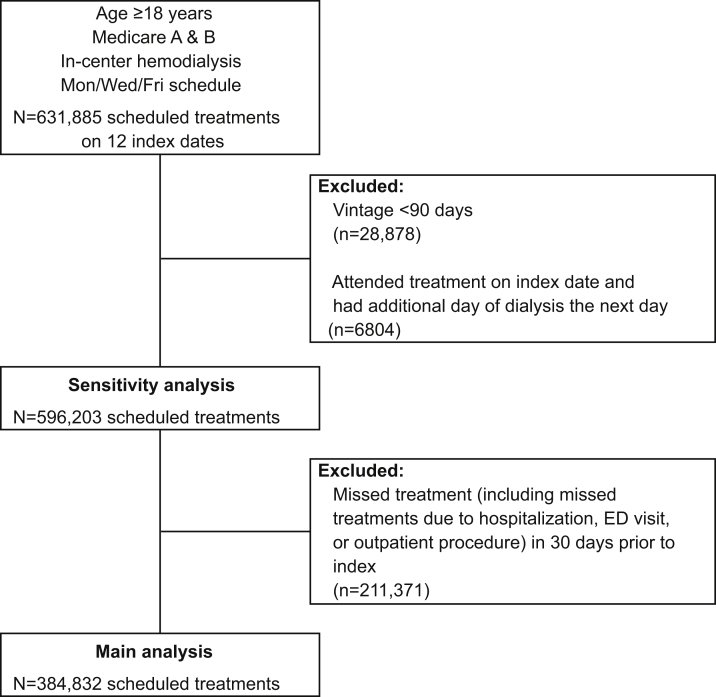
Setting & participants: Included patients were those who were, as of any of 12 index dates during 2014, adult Medicare beneficiaries treated with in-center HD (vintage ≥ 90 days) on a Monday/Wednesday/Friday schedule.
Exposure: Treatment attendance on the index date and the subsequent day.
Outcomes: Hospital admissions, emergency department visits, mortality, blood pressure, and anemia measures, considered during the 7- and 30-day periods following exposure.
Analytical approach: In parallel analyses, patients who missed or rescheduled treatment were each matched (1:5) to patients who attended treatment on the index date on the basis of index day of week and propensity score. Within the matched cohorts, outcomes were compared across exposures using repeated-measures generalized linear models.
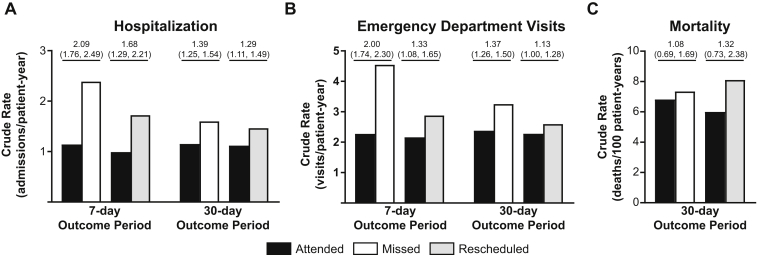
Results: Compared with attending treatment (N = 19,260), a missed treatment (N = 3,852) was associated with a 2.09-fold higher rate of hospitalization in the subsequent 7 days; a rescheduled treatment (N = 2,128) was associated with a 1.68-fold higher rate of hospitalization than attending (N = 10,640). Compared with attending treatment, hospitalization rates were 1.39- and 1.28-fold higher among patients who missed and rescheduled treatment, respectively, during the 30-day outcome period. Emergency department visits followed a similar pattern of associations as hospitalization. No statistically significant associations were observed with respect to mortality for either missed or rescheduled treatments compared with attending treatment.
Limitations: Possible influence of unmeasured confounding; unknown generalizability to patients with non-Medicare insurance.
Conclusions: Attending a rescheduled in-center HD treatment attenuates but does not fully mitigate the adverse effects of a missed treatment.
Keywords: adherence; hemodialysis; outcomes; treatment attendance.
© 2019 The Authors.
Figures

Comment in
-
Does Rescheduling a Missed In-Center Hemodialysis Treatment Improve Clinical Outcomes?Kidney Med. 2020 Feb 1;2(1):3-4. doi: 10.1016/j.xkme.2020.01.004. eCollection 2020 Jan-Feb. Kidney Med. 2020. PMID: 32734942 Free PMC article. No abstract available.
References
-
- Al Salmi I., Larkina M., Wang M. Missed hemodialysis treatments: international variation, predictors, and outcomes in the Dialysis Outcomes and Practice Patterns Study (DOPPS) Am J Kidney Dis. 2018;72(5):634–643. - PubMed
LinkOut - more resources
Full Text Sources
