

The Virtual Spine Examination: Telemedicine in the Era of COVID-19 and Beyond
- PMID: 32734784
- PMCID: PMC8258829
- DOI: 10.1177/2192568220947744
The Virtual Spine Examination: Telemedicine in the Era of COVID-19 and Beyond
Abstract
Study design: Narrative review.
Objectives: Describe a comprehensive spine telemedicine examination.
Methods: We discuss telemedicine examination techniques for commonly encountered spine conditions.
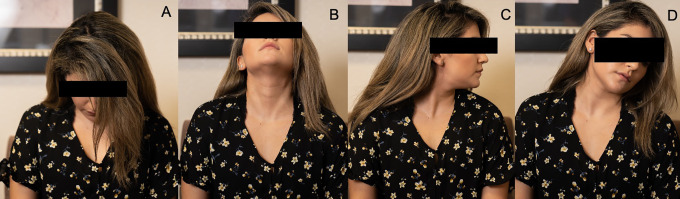
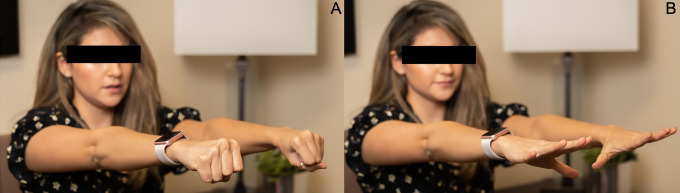
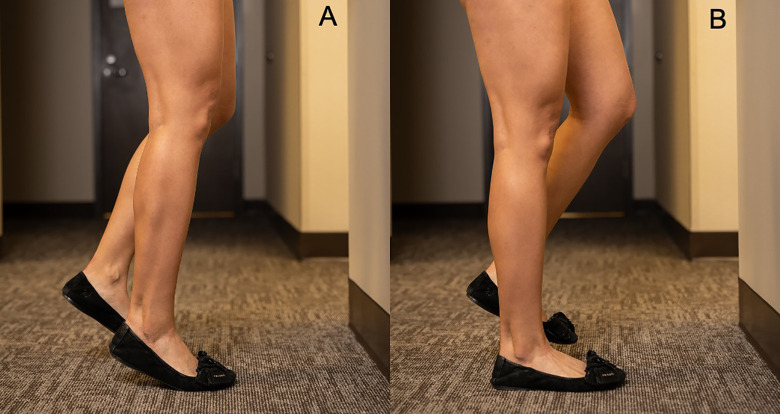
Results: Techniques to evaluate gait, the cervical spine, the lumbar spine, adult spinal deformity patients, and adolescent scoliosis patients via telemedicine are described. We review limitations of the spine telemedicine examination and discuss special considerations such as patient safety and criteria for in-person assessment.
Conclusions: While there are limitations to the spine telemedicine examination, unique strategies exist to provide important information to the examiner. Efforts have already been undertaken to validate and expand the capabilities of the spine telemedicine examination.
Keywords: COVID-19; telemedicine; virtual spine examination.
Conflict of interest statement
Figures






References
LinkOut - more resources
Full Text Sources
