

COVID-19-Associated Coagulopathy: An Exacerbated Immunothrombosis Response
- PMID: 32735131
- PMCID: PMC7401047
- DOI: 10.1177/1076029620943293
COVID-19-Associated Coagulopathy: An Exacerbated Immunothrombosis Response
Abstract
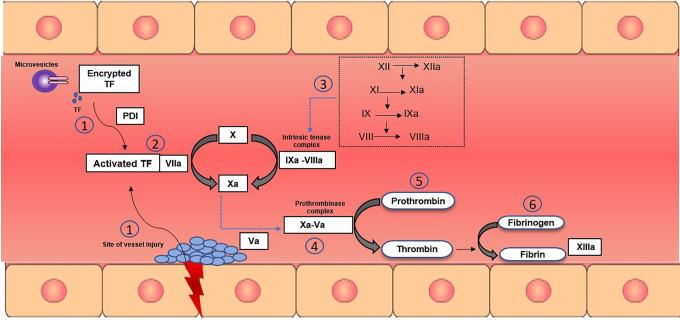
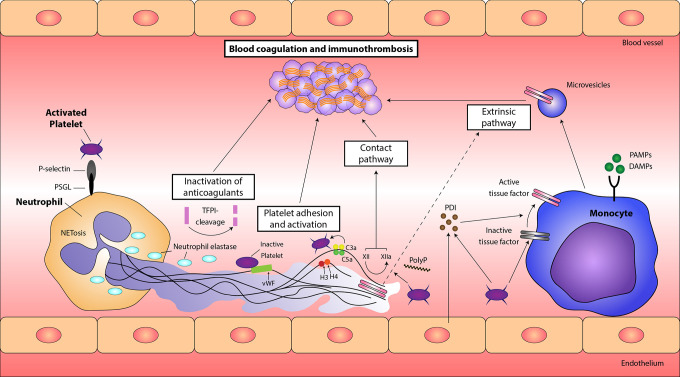
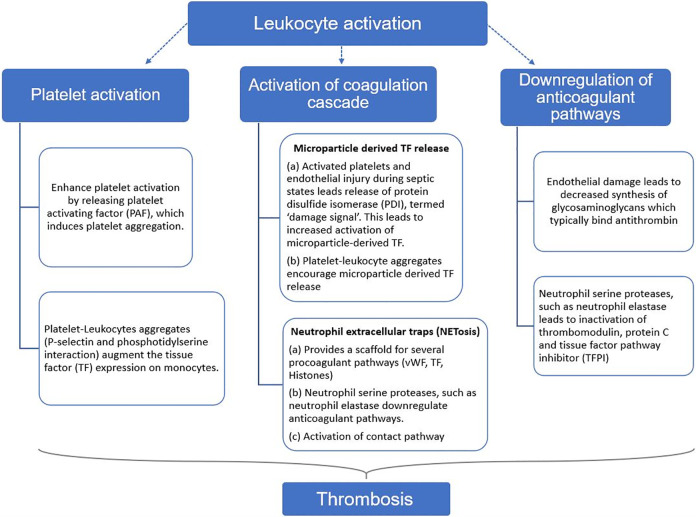
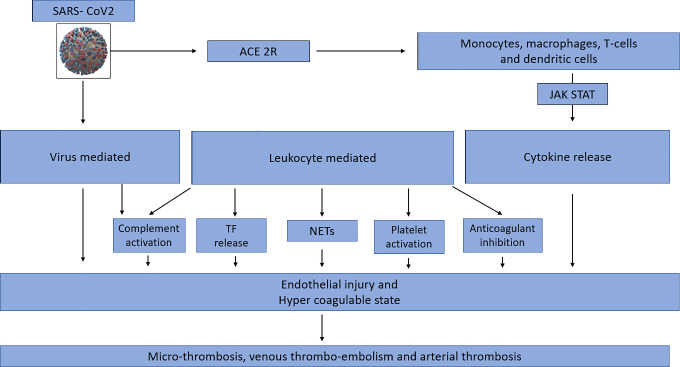
Since the onset of the global pandemic in early 2020, coronavirus disease 2019 (COVID-19) has posed a multitude of challenges to health care systems worldwide. In order to combat these challenges and devise appropriate therapeutic strategies, it becomes of paramount importance to elucidate the pathophysiology of this illness. Coronavirus disease 2019, caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV2), is characterized by a dysregulated immune system and hypercoagulability. COVID-associated coagulopathy (CAC) was recognized based on profound d-dimer elevations and evidence of microthrombi and macrothrombi, both in venous and arterial systems. The underlying mechanisms associated with CAC have been suggested, but not clearly defined. The model of immunothrombosis illustrates the elaborate crosstalk between the innate immune system and coagulation. The rendering of a procoagulant state in COVID-19 involves the interplay of many innate immune pathways. The SARS-CoV2 virus can directly infect immune and endothelial cells, leading to endothelial injury and dysregulation of the immune system. Activated leukocytes potentiate a procoagulant state via release of intravascular tissue factor, platelet activation, NETosis, and inhibition of anticoagulant mechanisms. Additional pathways of specific relevance in CAC include cytokine release and complement activation. All these mechanisms have recently been reported in COVID-19. Immunothrombosis provides a comprehensive perspective of the several synergistic pathways pertinent to the pathogenesis of CAC.
Keywords: COVID-19; coagulopathy; immunothrombosis.
Conflict of interest statement
Figures
References
-
- Munster VJ, Koopmans M, Doremalen NV, Riel DV, Wit ED. A novel coronavirus emerging in China—key questions for impact assessment. N Eng J Med. 2020;382(8):692–694. doi:10.1056/nejmp2000929 - PubMed
-
- Engelmann B, Massberg S. Thrombosis as an intravascular effector of innate immunity. Nat Rev Immunol. 2012;13(1):34–45. doi:10.1038/nri3345 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
